

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
Mecnoium obstruction in very low birth weight infants (VLBWI), which delays enteral feeding and is one of the major causes of bowel obstruction, can be diagnosed and treated with hyperosmolar water-soluble contrast enema. The purpose of this study was to observe the clinical findings of meconium obstruction, the improvement of small bowel obstruction after contrast enema, and the complications related to the enema.
Methods
Hypersolmolar water-soluble contrast enemas were performed in 14 VLBWIs with meconium obstruction. Clinical findings, radiologic findings, feeding intolerance, effectiveness, and complications of enemas were observed. Also, clinical findings related to meconium obstruction were compared with 18 VLBWIs without meconium obstruction.
Results
1) Fourteen VLBWIs with meconium obstruction had significantly lower 5 minutes Apgar scores than 18 VLBWIs without meconium obstruction (p<0.05). Moreover, the day of last meconium passing, and the day of the first trial and full enteral feeding were delayed significantly. 2) A total of 18 enemas were performed in the 14 infants. The contrast medium passed the ileocecal valve and reached the terminal ileus in 12 enemas. Of the 12 enemas, 11 were successful, but 1 infant underwent an ileotomy, even though the contrast medium reached the terminal ileum. 3) Intestinal obstruction was not relieved in three of five infants, in whom the contrast medium failed to pass the ileocecal valve. Obstruction was relieved after repeated enemas in which the contrast medium reached the terminal ileum. 4) No complications associated with water-soluble contrast enemas were observed.
Figures and Tables
Table 1
Comparison of Perinatal and Neonatal Characteristics between Infants with and without Meconium Obstruction

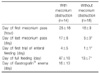
Table 2
Comparison of Meconium Passage and Feeding between Infants with and without Meconium Obstruction


References
1. Shinohara T, Tsuda M, Koyama N. Management of meconium-related ileus in very low-birthweight infants. Pediatr Int. 2007. 49:641–644.

2. Durkin EF, Shaaban A. Commonly encountered surgical problems in the fetus and neonate. Pediatr Clin North Am. 2009. 56:647–669.
3. Garza-Cox S, Keeney SE, Angel CA, Thompson LL, Swischuk LE. Meconium obstruction in the very low birth weight premature infant. Pediatrics. 2004. 114:285–290.
4. Emil S, Nguyen T, Sills J, Padilla G. Meconium obstruction in extremely low-birth-weight neonates: guidelines for diagnosis and management. J Pediatr Surg. 2004. 39:731–737.
5. Haiden N, Jilma B, Gerhold B, Klebermass K, Prusa AR, Kuhle S, et al. Small volume enemas do not accelerate meconium evacuation in very low birth weight infants. J Pediatr Gastroenterol Nutr. 2007. 44:270–273.
6. Burke MS, Ragi JM, Karamanoukian HL, Kotter M, Brisseau GF, Borowitz DS, et al. New strategies in nonoperative management of meconium ileus. J Pediatr Surg. 2002. 37:760–764.
7. Winfield RD, Beierle EA. Pediatric surgical issues in meconium disease and cystic fibrosis. Surg Clin North Am. 2006. 86:317–327.
8. Siegel MJ, Shackelford GD, McAlister WH. Neonatal meconium blockage in the ileum and proximal colon. Radiology. 1979. 132:79–82.
9. Krasna IH, Rosenfeld D, Salerno P. Is it necrotizing enterocolitis, microcolon of prematurity, or delayed meconium plug? A dilemma in the tiny premature infant. J Pediatr Surg. 1996. 31:855–858.
10. Jawaheer J, Khalil B, Plummer T, Bianchi A, Morecroft J, Rakoczy G, et al. Primary resection and anastomosis for complicated meconium ileus: a safe procedure? Pediatr Surg Int. 2007. 23:1091–1093.
11. Noblett HR. Treatment of uncomplicated meconium ileus by Gastrografin enema: a preliminary report. J Pediatr Surg. 1969. 4:190–197.
12. Shim SY, Kim HS, Kim DH, Kim EK, Son DW, Kim BI, et al. Induction of early meconium evacuation promotes feeding tolerance in very low birth weight infants. Neonatology. 2007. 92:67–72.
13. Mihatsch WA, Franz AR, Lindner W, Pohlandt F. Meconium passage in extremely low birthweight infants and its relation to very early enteral nutrition. Acta Paediatr. 2001. 90:409–411.
14. Caniano DA, Beaver BL. Meconium ileus: a fifteen-year experience with forty-two neonates. Surgery. 1987. 102:699–703.
15. Amodio J, Berdon W, Abramson S, Stolar C. Microcolon of prematurity: a form of functional obstruction. AJR Am J Roentgenol. 1986. 146:239–244.
16. Kenny SE, Vanderwinden JM, Rintala RJ, Connell MG, Lloyd DA, Vanderhaegen JJ, et al. Delayed maturation of the interstitial cells of Cajal: a new diagnosis for transient neonatal pseudoobstruction. Report of two cases. J Pediatr Surg. 1998. 33:94–98.
17. Goo HW, Kim KS, Kim AR, Pi SY, Yoon CH. Sonography-guided Gastrografin Enema for Meconium Plug Syndrome in Premature Newborns: Preliminary Results. J Korean Radiol Soc. 2004. 50:281–288.
18. Park HS, Kim TH, Kim HY, Park JH. Three cases of meconium plug syndrome. Korean J Pediatr Gastroenterol Nutr. 2006. 009:249–255.
 XML Download
XML Download