

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
Ultrasonography (US) is widely used as a screening test in patients with abdominal pain (AP). We investigated the usefulness of US by a pediatrician in children with AP.
Methods
We retrospectively analysed the medical records of children with AP who undertook US from December, 2008 to July, 2010.
Results
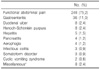
A total of 628 patients (325 male, 303 female) were enrolled in this study. The mean age of patients was 8.08±4.61 years. Duration of AP was acute in 427 and chronic in 201 patients. Localization of AP was diffuse (36.9%), periumbilical (24.4%), epigastric (21.0%), and right lower quadrant (8.1%). On the examination, there were no abnormal findings in 327 patients (52.1%). Abnormal ultrasonographic findings were mesenteric lymphadenitis (27.1%), intestinal mural thickening (10.0%), intussusception (3.0%), appendicitis (2.6%), choledochal cyst (1.6%), and pancreatitis (0.3%). We performed additional imaging studies such as computed tomography (CT) or magnetic resonance imaging (MRI) in 39 patients who showed obscure findings on the US. In 33 patients (84.6%), the same results were obtained from CT or MRI. Two cases of appendicitis, one case of pancreatitis and one case of Henoch-Shönlein purpura were diagnosed by the CT examination. However, there were two cases of appendicitis diagnosed by US thathad no evidence of appendicitis on the CT. Diagnostic accuracy of initial US in children with abdominal pain was 99.4%.
Figures and Tables
 | Fig. 1Localization of abdominal pain. RLQ: right lower quadrant, RUQ: right upper quadrant, LLQ: left lower quadrant, LUQ: left upper quadrant.
|



References
1. Lim JH, Lee SJ. Ultrasonography of the acute abdomen. J Korean Med Assoc. 2007. 50:73–79.

2. Middleton WD, Siegel MJ. Siegel MJ, editor. Physical principles and instrumentation. Pediatric sonography. 2002. 3rd ed. Philadelphia: Lippincort Williams & Wilkins;1–20.
3. Choi BI. Ultrasound diagnosis of the abdomen. 2006. 1st ed. Seoul: Ilchokak;363–394.
4. Bae SI, Park JH. Analysis of 1,000 cases of abdominal ultrasonography performed by a pediatrician. Korean J Pediatr Gastroenterol Nutr. 2007. 10:28–35.
5. Ahn SJ, Kho CY, Kim DU, Shin TY, Lee SS, Kim YS, et al. Emergency abdominal ultrasonography for differential diagnosis of acute abdominal pain: COUCH (complaint-oriented ultrasonography with check list) approach. J Korean Soc Emerg Med. 2008. 19:114–124.
6. Lee SW, Lee HK, Lee TW, Oh YH, Kim S, Lee CY. Mesenteric lymphadenitis and acute abdomen in children: correlation between sonographic findings and clinical symptom. J Korean Radiol Soc. 1995. 33:647–651.
7. Di Lorenzo C, Colletti RB, Lehmann HP, Boyle JT, Gerson WT, Hyams JS, et al. Chronic abdominal pain in children: a clinical report of the American Academy of Pediatrics and the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition. J Pediatr Gastroenterol Nutr. 2005. 40:245–248.
8. Hudson PA, Promes SB. Abdominal ultrasonography. Emerg Med Clin North Am. 1997. 15:825–848.
9. Karmazyn B, Werner EA, Rejaie B, Applegate KE. Mesenteric lymph nodes in children: what is normal? Pediatr Radiol. 2005. 35:774–777.
10. Lee TH, Hong YR, Yeon GM, Lee JW, Park JH. Clinical features of infectious ileocecitis in children. Korean J Pediatr Gastroenterol Nutr. 2010. 13:30–35.
11. Smith DE, Kirchmer NA, Stewart DR. Use of the barium enema in diagnosis of acute appendicitis and its complications. Am J Surg. 1979. 138:829–834.
12. Lee MK, Im CS, An SM, Kim CH, Lee DJ, Kwon JH. Ultrasonography for diagnosis of acute appendicitis in children. J Korean Pediatr Soc. 1996. 39:497–502.
13. Vignault F, Filiatrault D, Brandt ML, Garel L, Grignon A, Ouimet A. Acute appendicitis in children: an evaluation with ultrasound. Radiology. 1990. 176:501–504.
14. Ramachandran P, Sivit CJ, Newman KD, Schwartz MZ. Ultrasonography as an adjunct in the diagnosis of acute appendicitis: a 4-year experience. J Pediatr Surg. 1996. 31:164–189.
15. Suh HS, Chung MH, Kim KT. Ultrasonography for the acute appendicitis. J Korean Radiol Soc. 1987. 23:998–1007.
16. Lee JD, Lee JT, Cho JW, Yang JY. Diagnosis of acute appendicitis by ultrasonography. J Korean Soc Med Ultrasound. 1987. 6:158–167.
17. Abu-Yousef MM, Bleicher JJ, Maber JW, Urdaneta LF, Franker FA, Metcalf AM. High-resolution sonography of acute appendicitis. AJR Am J Roentgenol. 1987. 149:53–58.
18. Rubin SZ, Martin DJ. Ultrasonography in the management of possible appendicitis in childhood. J Pediatr Surg. 1990. 25:737–740.
19. Roosevelt GE, Reynolds SL. Does the use of ultrasonography improve the outcome of children with appendicitis? Acad Emerg Med. 1998. 5:1071–1075.
20. Ong EMW, Venkatesh SK. Ascending retrocecal appendicitis presenting with right upper abdominal pain: Utility of computed tomography. World J Gastroenterol. 2009. 15:3576–3579.
 XML Download
XML Download