

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Retroperitoneal cystic lymphangiomas are benign, extremely rare tumors. Although surgical resection is the treatment of choice, sclerotherapy should be considered initially. A 9-year-old boy was admitted due do worsening abdominal pain of 4 days duration. Serial complete blood counts revealed a hemoglobin level of 12.8 g/dL on admission to 10.6 g/dL on hospital day 3. An abdominal computed tomography (CT) scan showed a large, lobulated, septated, retroperitoneal cystic mass (10×9.5×5 cm) in the left anterior pararenal space with intracystic hemorrhage surrounding the inferior mesenteric vein (IMV). Because of the high operative risk, we performed a tubogram of the cystic mass, percutaneous catheter drainage (PCD), and ethanol sclerotherapy. The follow-up abdominal CT scan showed that the cystic mass had decreased in size. He is well without relapse of the retroperitoneal cystic mass for 13 months after discharge. Sclerotherapy with PCD should be considered as initial therapy for patients with retroperitoneal cystic lymphangiomas at high surgical risk.
Figures and Tables
 | Fig. 1On admission, an abdominal CT scan showed a large, lobulated, septated, retroperitoneal cystic mass (10×9.5×5 cm [arrowheads]) in the left anterior pararenal space with intracystic hemorrhage (*) surrounding the inferior mesenteric vein (IMV [small arrow]).
|
 | Fig. 2On hospital day 3, a T2-weighted MR scan showed the cystic mass had increased in size with hemorrhage. The hemoglobin level had changed to 10.5 g/dL.
|
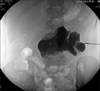
 | Fig. 3On hospital day 6, a tubogram was performed. The contrast media leaked out to the left paracolic gutters.
|

References
1. Okazaki T, Iwatani S, Yanai T, Kobayashi H, Kato Y, Marusasa T, et al. Treatment of lymphangioma in children: our experience of 128 cases. J Pediatr Surg. 2007. 42:386–389.

2. de Perrot M, Rostan O, Morel P, Le Coultre C. Abdominal lymphangioma in adults and children. Br J Surg. 1998. 85:395–397.
3. Hancock BJ, St-Vil D, Luks FI, Di Lorenzo M, Blanchard H. Complications of lymphangiomas in children. J Pediatr Surg. 1992. 27:220–224. discussion 4-6.
4. Steyaert H, Guitard J, Moscovici J, Juricic M, Vaysse P, Juskiewenski S. Abdominal cystic lymphangioma in children: benign lesions that can have a proliferative course. J Pediatr Surg. 1996. 31:677–680.
5. Konen O, Rathaus V, Dlugy E, Freud E, Kessler A, Shapiro M, et al. Childhood abdominal cystic lymphangioma. Pediatr Radiol. 2002. 32:88–94.
6. Davidson AJ, Hartman DS. Lymphangioma of the retroperitoneum: CT and sonographic characteristic. Radiology. 1990. 175:507–510.
7. Roisman I, Manny J, Fields S, Shiloni E. Intra-abdominal lymphangioma. Br J Surg. 1989. 76:485–489.
8. Yang DH, Goo HW. Generalized lymphangiomatosis: radiologic findings in three pediatric patients. Korean J Radiol. 2006. 7:287–291.
9. Shankar KR, Roche CJ, Carty HM, Turnock RR. Cystic retroperitoneal lymphangioma: treatment by image-guided percutaneous catheter drainage and sclerotherapy. Eur Radiol. 2001. 11:1021–1023.
10. Kosumi T, Kubota A, Yonekura T, Yamauchi K. Cystic lymphangioma of Retzius space manifested as acute abdomen. Eur J Pediatr Surg. 2006. 16:120–122.
12. Yang DM, Jung DH, Kim H, Kang JH, Kim SH, Kim JH, et al. Retroperitoneal cystic masses: CT, clinical, and pathologic findings and literature review. Radiographics. 2004. 24:1353–1365.
13. Iyer R, Eftekhari F, Varma D, Jaffe N. Cystic retroperitoneal lymphangioma: CT, ultrasound and MR findings. Pediatr Radiol. 1993. 23:305–306.
14. de Lagausie P, Bonnard A, Berrebi D, Lepretre O, Statopoulos L, Delarue A, et al. Abdominal lymphangiomas in children: interest of the laparoscopic approach. Surg Endosc. 2007. 21:1153–1157.
15. Tran Ngoc N, Tran Xuan N. Cystic hygroma in children: a report of 126 cases. J Pediatr Surg. 1974. 9:191–195.
16. Luzzatto C, Midrio P, Tchaprassian Z, Guglielmi M. Sclerosing treatment of lymphangiomas with OK-432. Arch Dis Child. 2000. 82:316–318.
17. Park SW, Cha IH, Kim KA, Hong SJ, Park CM, Chung HH. Percutaneous sclerotherapy using acetic acid after failure of alcohol ablation in an intra-abdominal lymphangioma. Cardiovasc Intervent Radiol. 2004. 27:285–287.
18. Ozdemir H, Kocakoc E, Bozgeyik Z, Cobanoglu B. Recurrent retroperitoneal cystic lymphangioma. Yonsei Med J. 2005. 46:715–718.
19. Fujino A, Moriya Y, Morikawa Y, Hoshino K, Watanabe T, Shimojima N, et al. A role of cytokines in OK-432 injection therapy for cystic lymphangioma: an approach to the mechanism. J Pediatr Surg. 2003. 38:1806–1809.
20. Dubois J, Garel L, Abela A, Laberge L, Yazbeck S. Lymphangiomas in children: percutaneous sclerotherapy with an alcoholic solution of zein. Radiology. 1997. 204:651–654.
21. Tanaka K, Inomata Y, Utsunomiya H, Uemoto S, Asonuma K, Katayama T, et al. Sclerosing therapy with bleomycin emulsion for lymphangioma in children. Pediatr Surg Int. 1990. 5:270–273.
22. Molitch HI, Unger EC, Witte CL, vanSonnenberg E. Percutaneous sclerotherapy of lymphangiomas. Radiology. 1995. 194:343–347.
 XML Download
XML Download