

 PDF
PDF ePub
ePub Citation
Citation Print
Print



서론
국내에서 신생아집중치료실(neonatal intensive care unit, NICU)이 개설되고 신생아용 인공호흡기 및 감시장치 등을 사용하여 본격적으로 신생아중환자 치료가 이루어지기 시작한 것은 1980년대부터이다. 이후 1990년대에 들어와 인공폐표면활성제가 사용되었고, 전국적으로 NICU 시설이 확대되었으며 1993년 대한신생아학회가 창립된 이후 신생아학회 주도로 신생아 관리 및 치료가 교육되고, 발전되는 전기를 맞았다. 2000년대에 들어서는 고빈도 인공환기법, 흡입일산화질소 사용 등 새로운 신생아 치료방법과 기구들이 도입되고 NICU 관리에 대하여 정부의 각종 제도적 보완이 이루어졌다[123].
한국 전국자료에서 미숙아 생존의 중요지표인 출생체중 1,500 g 미만의 극소저체중출생아(very low birth weight infant, VLBWI)의 생존율은 1980년대 불과 38.3%에서 2014년 84.8%로 크게 개선되었으며 같은 시기 초극소저체중출생아(extremely low birth weight infants, ELBWI)의 생존율은 12.3%에서 69.6%로 늘었다[34]. 이러한 결과는 한국의 신생아사망률과 영아사망률의 개선에도 영향을 미쳐서, 한국의 신생아사망률은 1993년 6.6에서 2010년 3.2로 크게 감소되었다[5]. 이렇듯 한국에서 NICU가 본격적으로 운영되기 시작한 이후 불과 30년 동안 신생아 치료 성적의 변화는 빠르게 이루어져서 이제는 다른 선진국과 비견할 만큼 발전되어있다[5]. 미숙아 혹은 저체중출생아, VLBWI에서 잘 발생하는 질환의 한국 전체에서의 빈도를 파악하는 것은 치료나 역학에서 중요한 사항이다. 그러나 이들 그룹에서 잘 발병하는 질병이환율에 관한 보고는 그 동안 병원 단위나 지역 단위에 국한된 단편적인 보고들에 불과하였고, 한국 전체를 나타내는 전국 규모의 질병이환율의 보고는 미비한 상태였다[6].
대한신생아학회에서는 2013년 4월 15일, 질병관리본부와 국립보건연구원과 함께 전국적인 규모로 전국 NICU의 VLBWI의 등록, 자료분석, 교육, 질 관리, 질병이환율 및 사망률 보고 등을 담당할 한국신생아네트워크(Korean Neonatal Network, KNN)를 발족하였으며[7], 2016년 4월 현재 64개의 전국 대다수의 NICU가 참여하여 6,700여 명의 환아가 등록되고 있다. 자료수집은 환자 퇴원 시점인 단기등록과 교정연령 18-24개월과 만 3세 외래방문시점인 장기추적등록으로 구분된다. 향후 KNN 네트워크를 이용한 미숙아 관련 질환의 질병이환율, 사망률 및 치료에 대한 반응 등에 대한 전국적 자료의 제시 및 분석이 가능해졌다. 또한 KNN 네트워크의 규모와 구성은 일본의 Neonatal Research Network나 미국의 National Institute of Child Health and Human Development Neonatal Research Network와 Vermont-Oxford Neonatal Research Network의 기능과 유사하여 운영이 잘 이루어지면 한국을 대표하는 자료를 제공하고 나아가서 외국과의 비교에도 유용하게 쓰일 것이다[78]. 본 리뷰에서는 2013년부터 2014년 기간 KNN에 등록된 전국 55개 NICU의 2,386명의 자료를 분석하여 발표한 논문들의 결과를 기준으로 최근 우리나라의 VLBWI의 사망률의 변화 및 주요 질병이환율을 알아보았다.
극소저체중출생아 생존율의 변화
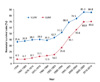
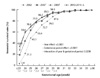
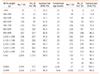
한국 신생아생존율 중 1,500 g 미만의 국내 VLBWI 생존율의 변화를 보면 1980년 이전까지 큰 차이 없이 답보상태에 있다가 1980년대 후반기부터 급속히 증가하여 2009년 85.3%로 증가하였으며 같은 시기 1,000 g 미만 ELBWI생존율은 12.3%에서 68.9%로 증가하였다(Figure 1) [3]. 이러한 결과는 재태주수에 따른 생존율의 시기별 변화에서도 나타난다(Figure 2) [23]. Shim 등[3]이 2013년부터 2014년 기간 출생하여 KNN에 등록된 2,386 명의 VLBWI를 대상으로 한 연구에 따르면 이 기간 NICU에서 치료 받은 후 생존하여 퇴원한 VLBWI는 84.8%였으며 ELBWI는 69.6%였다. 같은 논문에서 재태주수에 따른 생존율의 변화는 24주 이하의 생존율은 2002년 21.3%에 비하여 2014년 59.6%로, 같은 기간 28주는 79%에서 89.5%로 향상되었으며 29주 이상의 경우 최근에는 95% 이상의 높은 생존율을 보인다고 보고하였다[2391011]. 출생체중에 따른 최근의 생존율도 500 g 미만은 40.4%로 낮았으나 500-749 g에서 55.4%로 증가하였고 750 g 이상에서는 생존율이 81.3%로 더욱 향상되어 출생체중 1,000 g이상 대부분의 환아가 생존하였다(Table 1) [3]. 이와 같은 생존율은 비슷한 기간 동안 발표된 캐나다, 호주, 유럽연합의 미숙아 재태주수와 출생체중에 따른 생존율에 근접하는 좋은 치료성적을 보였다. 하지만 세계 최고수준인 일본의 성적에는 미치지 못하는 것으로 나타났다(Figure 3) [312131415].
Lim 등[16]은 KNN 데이터를 이용하여 VLBWI의 NICU 치료기간 동안의 사망원인의 가장 주된 원인을 기준으로 순환계통과 호흡계, 소화계, 감염, 신경계, 선천성기형, 기타의 원인 6가지로 나누어 분석한 결과를 보고하였는데 NICU치료 중 사망한 원인으로 순환계통 및 호흡계통이 44.2%로 가장 많았으며 감염이 18.4%, 소화계통이 13.4%인 것으로 나타났으며 재태주수와 출생체중에 따라 분류하여도 이러한 사망원인 순위에는 큰 차이가 없었다고 하였다.
극소저체중출생아 질병이환율의 변화
Kim 등[6]은 전국의 97개 신생아중환자실에서 2012년
6월 출생한 신생아들 중 976명의 저체중출생아 및 VLBWI 신생아들의 의무기록을 연구하여 보고한 한국보건사회연구원의 보고서[17]를 인용하여 국내 VLBWI의 유병률을 연구보고하였다. 연구결과 251명의 VLBWI에서의 빈도 순에 따른 유병률은 신생아호흡곤란증후군(respiratory distress syndrome) 78.9%, 신생아황달 57.4%, 동맥관개존(patent ductus arteriosus, PDA) 51.0%, 무호흡증 45.4%, 패혈증 23.9%, 미숙아만성폐질환(bronchopulmonary dysplasia, BPD) 21.1%, 부당경량아 17.5% 등의 순이었다. Kim 등[6]은 이전의 보고들이 단편적인 보고들에 불과하여 한국 전체를 나타내는 전국 규모의 질병이환율의 보고가 매우 미비한 상태임을 설명하였다. 이에 대하여 2015년에는 2013년부터 2014년 기간 KNN에 등록된 전국 55개 NICU의 2,386명의 자료를 분석한 논문들이 발표되었으며 이들 결과들은 최근의 한국 VLBWI들의 주요 질병에 대한 유병률 및 특성을 대표할 수 있을 것으로 생각되어 아래에 정리해 보았다.
1. 미숙아만성폐질환
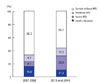
BPD는 교정나이 36주가 되는 시점에도 계속 산소치료나 인공호흡기치료가 필요한 경우에 진단하게 된다. 2007년
부터 2008년 기간 이루어진 전국규모의 통계에서 Choi 등[18]은 77개 NICU의 VLBWI 혹은 임신나이 32 주 이전의 3,841명의 출생아를 대상으로 조사하였을 때, BPD는 18.0% 그리고, BPD 혹은 사망은 37.0%로 보고하였다. 이후 Jo 등[19]은 2013부터 2014년 기간 2,386명의 KNN 데이터를 이용한 연구에서 생존한 VLBWI에서 BPD로 진단받은 경우는 28.9%였고, 30% 이상의 높은 농도의 산소가 필요한 중증의 빈도는 7.8%, 교정 나이 36주 시점에도 기관 삽관을 한 채로 인공호흡기치료를 받았던 경우가 7.1%로 보고하였다 (Figure 4) [101819]. Jo 등[19]은 2007년부터 2014년 기간 BPD 발생률은 18.0%에서 28.9%로 늘었으나 이 시기 NICU에서의 사망률은 18.8%에서 12.9%로 줄어든 것을 고려하면 BPD 발생률이 늘어난 이유가 VLBWI 생존율이 증가함에 따라 생존한 BPD 환아가 늘어났기 때문으로 보고하였다.
2. 뇌실내출혈 및 뇌실주위백질연화증
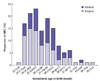
미숙아들에서 뇌실 주위의 뇌혈관 조직들이 성숙하지 못하고 취약하여, 뇌실내로 출혈이 일어나는 것을 미숙아 뇌실내출혈(intra-ventricular hemorrhage, IVH)이라고 한다. 미숙아 IVH는 그 출혈양상에 따라서 1기부터 4기까지의 단계가 있다. 특히 3기와 4기의 중증 IVH는 매우 심각하여 뇌수두증 및 장기간의 신경학적 장애와 같은 합병증을 유발할 가능성이 높아진다. Ahn 등[20]이 2013-2014년 기간 2,386명의 VLBWI의 KNN 자료를 이용하여 보고한 결과는 VLBWI 중에서 미숙아 IVH는 42.2%에서 발생하였으며 그들 중 IVH 3기 및 4기의 중증 IVH의 비율은 4.9%, 6.4%이었다. 또한 재태주수가 어릴수록 출혈 발생 비율이 높고 중증 출혈 비율이 높은 경향을 보인다고 하였다(Figure 5) [20].
뇌실주위백질연화증(periventricular leukomalacia, PVL)은 뇌실 주변에 위치한 뇌의 백질 조직이 괴사 및 손상되는 질병으로 미숙아에서 주로 나타나며 향후 운동 및 인지기능장애와 밀접한 관련성이 있다. Ahn 등[20]이 PVL 발병률에 관한 KNN 데이터를 이용한 연구에서 VLBWI 전체에서의 PVL 빈도는 8.3%였으며 IVH와는 달리 출생주수에 따라서 빈도가 달라지는 뚜렷한 상관관계는 보이지 않았다고 보고하였다.
3. 동맥관개존
태아기에 태반에서 산소를 공급받은 혈액은 폐를 거치지 않고 동맥관을 통하여 바로 태아의 하행대동맥을 거쳐서 태아에게 전신으로 산소를 공급하도록 되어있다. 동맥관은 출생 후 수시간 내에 기능적으로 닫히게 되고 해부학적으로는 수주 이내에 닫히게 된다. 미숙아의 경우 동맥관이 바로 닫히지 않고 열린 상태로 유지되는 경우가 많아 전신으로 가야 할 혈액이 일부가 폐로 가게 되면서 전신 각 기관으로 가는 혈액 및 산소량이 상대적으로 부족하게 되고 폐로 가는 혈액이 과다하게 되어 여러 가지 병적 상황을 만들게 된다. Lee 등[21]이 2013-2014년 기간 2,386명의 VLBWI의 KNN 자료를 이용하여 보고한 결과에 따르면 증상이 있거나 치료를 필요로 하였던 PDA의 발병 비율은 전체 VLBWI의 47.1%였고 그들 중 약물치료만 받았던 경우는 36%, 수술치료는 12.2%에서 각각 시행되었다. 특히 수술적 치료는 재태주수 28주 이하 VLBWI에서 많이 시행되었다(Table 2) [21].
6. 미숙아망막증
미숙아망막증은 출생 시 망막의 혈관이 완전히 형성되지 않은 미숙아에서 출생 후 혈관형성과정에 장애가 발생하여 비정상적인 섬유혈관증식이 발생하는 대표적인 미숙아 망막질환으로 심한 경우 망막박리로 실명까지 초래될 수 있다. Hwang 등[24]이 2013-2014년 기간 2,386명의 VLBWI의 KNN 자료를 이용하여 보고한 결과는 검사를 받은 VLBWI 전체에서 33.5%에서 미숙아망막증이 발생했으며 재태주수 24주 이하에서 88.9%, 25-28주는 53.2%, 29-32주는 12.8%의 빈도로 감소하는 경향을 보였으며 33주 이상에서는 3.3%에서 발생하였다(Figure 7).
결론
2016년 2월 통계청이 발표한 2015년 출생·사망통계에 따르면, 지난해 출생아는 총 43만 8,700명으로 2014년(43만 5,400명)보다 0.8% 증가하였지만 여전히 한국의 출생아 수는 경제협력개발기구 국가 중 최하위에 머물러 있다[25]. 또한 여자 한 명이 평생 낳을 것으로 예상되는 평균 합계 출산율은 1970년대 이후 지속적인 감소추세에 있으며, 2015년에는 1.24명까지 떨어졌다. 우리나라는 2001년 이래로 15년째 합계 출산율이 1.3명 이하인 '초저출산' 사회로 분류되는 초저출산 상태가 지속되고 있다[25]. 이에 반하여 저체중 및 37주 미만으로 태어난 출생아 수는 꾸준히 증가하고 있다[252627]. 미숙아는 높은 사망률과 주요 합병증을 동반하여 큰 사회경제적인 부담이 될 수 있다. 따라서 출생 후 미숙아에 대한 집중치료를 시행하여 생존율을 높이고 합병증을 최소화하여 건강한 국민의 일원이 되게 하는 것은 국가적으로도 매우 중요한 사항이다.
VLBWI 생존율은 신생아 집중치료 수준의 지표이며 이들의 생존율 향상은 그만큼 신생아 집중치료의 수준이 향상되었다는 것을 의미한다. Shim 등[3]의 연구에 따르면 2013-2014년 기간인 최근 VLBWI와 ELBWI의 NICU에서 퇴원시까지의 생존율은 각각 84.8%와 69.6%였다. 이러한 생존율은 세계에서 가장 높은 생존율을 보이는 일본에 비하여는 낮지만 미국, 캐나다, 오스트리아, 유럽연합과 비견할만하다[23]. VLBWI생존율 이상으로 중요한 지표들은 VLBWI들의 질병이환율이다. 그러나 서론에서 언급하였듯이 그동안 국내에서는 이와 관련된 보고가 병원 단위나 지역 단위에 국한된 단편적인 보고들에 불과하였다. 본 리뷰에서는 2013년 4월부터 전국적으로 등록이 시작된 KNN 데이터들 중 2013년에서 2014년 기간 수집된 2,386명의 VLBWI 데이터를 연구하여 보고된 전국 규모의 논문들을 리뷰하여 한국의 VLBWI들의 최근 질병이환율 및 사망률과 이들 수치의 변화를 파악하고자 하였다. 추후 지속적인 KNN 데이터 축적을 통하여 이들 수치들이 어떻게 향상되어 가는지 알 수 있을 것으로 생각한다.
Peer Reviewers' Commentary
본 원고는 한국 신생아 치료성적의 변화를 극소저체중출생아 중심으로 체계적으로 기술한 종설 논문이다. 역학에 대한 자료는 2013년부터 2014년까지 한국신생아네트워크 등록 자료를 분석하여 발표한 논문들의 결과를 기준으로 하였으며, 극소저체중출생아 사망률의 변화 및 주요 질병이환율을 체계적으로 적절하게 제시하고 기술하였다. 초저출산국가인 우리나라에서 매년 증가하는 극소저출생체중아들에 대하여 이들의 생존율을 높이고 합병증을 최소화하여 미래에 건강한 국민의 일원이 되게 하는 것은 국가적으로 매우 중요한 사항이다. 이를 위하여 현재 상황을 정확히 알고 근거를 바탕으로 한 정책을 수립하여야 한다. 본 원고는 최근 상황에 대한 정확한 데이터를 외국과 비교하여 제시하고 있으며 향후 지속적인 한국신생아네트워크 데이터 축적을 통하여 신생아집중치료실의 생존율과 주요 질병이환율의 변화를 확인할 수 있게 하는 자료로서 매우 큰 의의를 지닌다고 판단된다.
[정리: 편집위원회]





 XML Download
XML Download