

 PDF
PDF ePub
ePub Citation
Citation Print
Print


서론
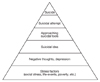
청소년 자살은 전세계적으로 중요한 사회 문제가 되고 있다. 자살은 죽음을 스스로 원해서 치명적인 행동을 통해 사망에 이른 것으로 정의할 수 있다[1]. 자살은 자살사고(suicidal idea)와 자살도구에 접근, 자살기도(suicidal attempt)를 거쳐 완료(completed suicide)에 이르는 일련의 과정으로 볼 수 있다[2] (Figure 1).
따라서, 자살로 사망한 경우에 그 20배에 달하는 자살기도자가 있으며[3], 훨씬 더 많은 청소년이 자해를 시도한 바 있음을 주목해야 한다[4]. 또한 한 명의 청소년이 자살을 했을 때 가족, 친구, 학생을 가르치는 교사, 이웃 등 많은 수가 큰 충격을 받게 되고 일부는 충격으로 외상후스트레스장애(posttraumatic stress disorder)를 경험하게 된다. 외상후스트레스장애는 우울증과 자살시도의 위험요인이 된다[5]. 이 밖에도 청소년 자살에는 성인과 다른 위험요인이 많이 있는데, 우울증, 충동성, 낮은 자존감 등 개인적인 요인 이외에 가정불화나 부모와의 갈등, 경제적 어려움과 같은 가정 요인, 학교폭력, 교우관계, 학업 스트레스와 같은 학교 요인, 미디어 영향, 주변인의 자살과 같은 사회적 요인 등이 위험요인이 된다[6]. 이러한 위험요인을 파악함으로써 청소년 자살의 예방과 조기 개입에 중요한 근거를 제시할 수 있다.
이 논문에서는 청소년 자살의 국내외 현황을 통계자료에 근거하여 고찰하고, 청소년 자살의 예방에 있어 중요한 위험요인을 검토하고자 한다.
청소년 자살률의 변화
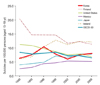
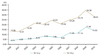
다른 OECD 국가들에서 15-19세 청소년 사망률이 전반적으로 감소추세를 보이는 것과는 달리 국내에서는 지속적인 증가추세를 보이고 있다(Figure 3). 미국에서는 1990년 이후로 청소년 자살률이 꾸준히 감소하고 있지만 OECD 평균보다는 높다. 미국에서 10-24세 사망원인의 3위가 자살이다. 총기류를 사용한 자살이 45%, 질식이 40%, 음독이 8%를 차지하고 있다[9].
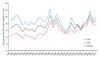
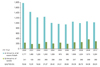
최근 결과인 2010년 국내 15-19세 청소년 자살률은 8.3/100,000으로 증가하였다. 특히, 여자에서 증가율이 남자보다 높은 것이 특징이다(Figure 4). 국내 15-19세 청소년의 사망자 절대 숫자는 지속적으로 감소하고 있으나, 사망원인 중 자살이 차지하는 상대적 비율은 지속적으로 증가하고 있다(Figure 5). 2000년 당시 청소년 사망원인 1위는 운수사고(교통사고)였고 자살은 2위였으나, 지난 10년간 운수사고로 인한 사망자는 감소한 반면, 자살로 인한 사망자는 계속 증가하였다[10]. 2009년의 경우, 15-24세 청소년의 사망원인 1순위는 자살(인구 10만 명당 15.3명)로 교통사고(8.4명)보다 두 배 가까이 높았고, 15-19세 청소년 사망원인 중 자살의 비중은 2000년 약 13.56%에서 2010년 약 28.24%로 두 배 이상 증가하였다(Figure 5).
최근 14세 이하 연령의 자살 통계도 파악되고 있는데, 자살이 1-14세 청소년의 사망원인 중 3위에 포함되고 있으며, 10-14세 아동청소년 사망원인 중 자살의 비율이 2000년 3.74%에서 2010년 14.63%로 4배 이상 증가하였다(Figure 6). 1-24세 인구의 사망 원인 1위가 자살로 집계되고 있어서 정책적 관심 및 대처가 필요하다.
2012년 한국보건의료연구원에서 2007-2009년 통계청 사망원인자료를 이용하여 12-18세 청소년의 십만 명당 자살률을 조사한 결과, 자살로 인한 사망자는 통계청 주민등록 연간인구자료 기준 742,816명 중 829명으로서 5.7/100,000이었고, 이중 남성은 5.8/100,000, 여성은 5.6/100,000이었다[11]. 연령대가 높은 15-18세에서는 8.2/100,000으로 연령대가 낮은 12-14세의 2.5/100,000에 비해 3배 이상 차이가 나며, 이는 OECD 국가의 15-19세 평균 자살률 6.8/100,000보다 높은 수준이었다. 연령에 따른 차이가 두드러지게 나타나므로, 학교를 기반한 자살예방사업에서는 고등학생 계층의 자살예방을 위해 더 노력해야 함을 알 수 있다.
2012년 한국보건의료연구원에서 2009년 청소년건강행태온라인조사 자료를 분석하여 청소년의 자살생각과 자살시도 현황을 살펴본 결과, 조사 대상자 57,009명 중 자살생각은 10,690명, 자살시도 경험은 2,376명으로 나타났다[11]. 제4기(2007-2009년) 국민건강영양조사 자료 중 청소년 연령대를 분석한 결과에서는 자살생각은 317명/2,133명, 자살시도는 17명/2,132명으로 나타났다. 종합해보면, 12-18세 청소년의 자살시도율은 4.44%, 평생 자살생각률 18.97%로 자살시도율은 자살률에 비해 772배(국외: 100-350배), 자살생각률은 3,328배 높았다[11]. 이는 자살을 고려하는 잠재적 위험군이 상당수 존재함을 시사한다.
청소년 자살 위험요인
이전의 연구에 의해 알려진 청소년 자살의 위험요인은 Table 1과 같다. 청소년 자살의 위험요인은 사회인구학적 요인, 정신건강 요인, 개인 및 가정적 요인으로 나누어 볼 수 있다. 정신건강문제인 우울증, 불안장애, 주의력결핍 과잉행동장애(attention deficit hyperactivity disorder, ADHD), 알코올 및 약물오남용의 문제가 자살과 연관되어 있다[4]. 자살방법에 쉽게 접근할 수 있는 것도 중요한 위험요인이 된다[9].
Renaud 등[12]은 캐나다의 퀘벡 지방에서 자살로 사망한 청소년 55명과 다른 이유로 사망한 청소년 55명에 대한 사후부검연구를 진행하였다. 두 군을 비교하였을 때 자살 사망군에서 우울증이 있는 경우가 48.4배 높았고, 충동조절장애가 13.6배 높았다. 이에 비해서 다른 정신질환은 자살과의 연관성이 낮게 나타났다. 이를 통해 우울증이 성인기뿐 아니라 청소년에서도 자살 사망의 주요한 원인임이 밝혀졌다.
Chronis-Tuscano 등[13]은 ADHD를 가진 청소년 125명과 대조군 123명을 장기추적관찰 하였다. 우울증과 자살시도가 초기 5년 간은 두 군에 차이가 없었으나 5년부터 13년 사이에 ADHD가 있는 군에서 유의한 증가를 나타내었다. 따라서 청소년기 ADHD가 향후 자살시도를 예측하는 위험요인이 된다고 하였다.
Aseltine 등[14]은 미국 메사추세츠 주의 웨슬리 지방에서 32,217명의 청소년을 대상으로 자살예방을 위한 Signs of Suicide (SOS) Program을 실시하였다. 심각한 음주가 청소년 자살의 중요한 위험요인이 되었고, 의사에 의해서 정기적으로 음주에 대한 평가를 하는 것이 자살위험을 가진 청소년을 발견하는데 도움이 되었다고 보고하였다.
Russell과 Joyner [15]는 미국 전역에서 11,840명의 청소년을 대상으로 성 정체성과 자살에 대한 연구를 진행하였다. 성적 소수자의 경우 자살에 대한 생각과 시도가 남녀 모두에서 2.5배 증가하는 것으로 파악되었다.
Glowinski 등[16]은 미주리 지역에서 쌍생아 3,416명에 대해 연구를 진행하였다. 쌍생아 중 한 명에서 자살기도를 하였을 때 일란성은 5.6배, 이란성은 4.0배 자살시도 위험이 증가하였다. 이로서 자살시도가 유전적인 영향을 받는다는 사실이 밝혀졌다.
국내에서 2012년 한국보건의료연구원이 청소년 자살의 위험요인에 대해 연구한 결과, 청소년 우울증 치료율(우울증 치료 중인 청소년 수/전체 청소년 인구수, %)을 청소년 자살률과 비교해 볼 때, 우울증 치료율이 자살률보다 더 낮은 것으로 나타났다. 청소년건강행태온라인조사 및 국민건강영양조사 자료분석에서도 우울증이 청소년 자살의 주요원인으로 나타난 점을 감안하면, 청소년 자살 생각 및 자살 시도의 가장 큰 위험요인은 우울증이라고 볼 수 있다. 따라서 청소년 우울증에 대한 체계적인 관리가 필요하다. 한편 스트레스 원인 중 교우관계와 가정형편이 주요한 위험요인으로 나타났으므로 학교폭력과 따돌림 문제를 해결하고 사회경제적 취약계층의 청소년 집단을 적극적으로 관리할 필요가 있다[11].
결론
청소년 자살은 서구 선진국에서는 감소하는 추세인데 반해서 한국에서는 증가하고 있으며, 특히 여아에서 증가 폭이 크다. 청소년 자살의 위험요인은 사회인구학적 요인, 정신건강 요인, 개인 및 가정적 요인으로 나누어 볼 수 있다. 정신건강 문제인 우울증, 불안장애, ADHD, 알코올 및 약물오남용의 문제를 조기에 발견해 치료하고, 부모가 제대로 돌보고 있는지 학대를 당하고 있는지 확인하고 도움을 제공하는 것이 청소년 자살률을 감소시키는데 중요하다고 할 수 있다.
현재 국내 여러 기관에서 청소년 자살률, 자살시도율, 자살생각률에 대한 조사가 이루어지고 있으나, 자살예방사업의 근거 확보를 위한 지속적이고 통합적인 자료는 확보되지 못하고 있으므로 범국가적인 종합대책의 일환으로 청소년 자살에 대한 정기적 실태조사가 필요하다. 이를 통해 청소년 자살관련 위험요인과 예방요인 및 상호관계에 대한 심층적인 연구가 필요하다.
Peer Reviewers' Commentary
이 논문에서는 청소년 자살의 국내외 현황을 통계 자료에 근거하여 고찰하였고, 청소년 자살의 위험요인을 검토하였다. 청소년 자살에는 성인과 다른 위험요인이 많이 있는데, 이들 위험요인을 파악하여 청소년 자살의 예방과 조기 개입을 위한 중요한 정책적 판단기준을 마련할 수 있을 것이다. 현재 국내 여러 기관에서 청소년 자살에 대한 조사가 이루어지고 있으나, 자살예방사업의 근거 확보를 위한 지속적이고 통합적인 자료는 확보되지 못하고 있는 상황이기 때문에 이들 연구를 종합하고 고찰하는 것은 중요한 작업이다. 결론적으로 소아와 청소년의 자살이 주된 사망원인으로 증가됨에 있어서 우울증을 포함한 정신질환과 스트레스의 조기 진단 및 조기개입의 중요성이 점점 더 커지고 있음을 보고하였다. 추후 전국적인 데이터베이스를 마련하고, 정기적인 추적관찰을 통해 청소년 자살관련 위험요인과 예방요인 및 상호관계에 대한 심층적인 연구가 필요하겠다.
[정리: 편집위원회]

 XML Download
XML Download