

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The population older than 65 years of the Korea was about 11.3% of the total population last year [1], and is expected to reach 24.3% and 38.2% in the year 2030 and 2050, respectively [2]. The proportion of elderly people to visit the hospital is increasing and laboratory tests are performed to screen them for many pathological conditions. The chemistry tests can be very important in diagnosis, especially for elderly people, in whom clinical symptoms and signs are not typical or often absent even during an acute event. Common reference intervals are needed for adequate interpretation of these tests. Since many chemistry markers change with age and the current reference intervals are mostly based on a population in the age range from 20 to 50 years, however, interpreting laboratory results from elderly people by the reference intervals for younger adults may not be appropriate [3-5]. Defining a 'healthy' elderly population and collecting data from them are difficult because diabetes, cancer, cardiovascular diseases, and some types of medication are common in older people. Therefore, reports of laboratory reference values for elderly people are sparse in Korea.
In this study, authors compared the distribution patterns of routine chemistry values from elderly people to younger adults to investigate if chemistry values change with aging and if present reference intervals are also valid to elderly people.
Materials and methods
1. Populations
From January, 2009 till June, 2011, The 2,604 Korean individuals above 65 years of age were selected from the people attending general health check-ups at Kyungpook National University Hospital. They were screened by using a health questionnaire that contained questions about medical history, present illness, and present medication and excluded from the final diagnosis of cancer, hyperlipidemia, diabetes, cardiovascular disease, viral hepatitis, and any past history of confirmed disease such as stroke. And some subjects were also excluded because of strong suspicion of disease from their laboratory data [3,6]: C reactive protein >200 mg/dL, blood urea nitrogen (BUN) >42 mg/dL, creatinine >2.6 mg/dL, total proteins >90 g/dL, glucose >180 mg/dL. Finally, 1,215 elderly people (group I) then consisted of 1,003 persons (551 males and 452 females) for 65 to 74 years (group Ia) and 212 persons (110 males and 102 females) older than 75 years (group Ib). 1,827 younger healthy adults (982 males and 845 females) below 65 years of age (mean age, 52.8 years; range, 21 to 64 years) (group II) were also evaluated as a comparing group. The study was approved by the institutional review board of Kyungpook National University Hospital and all the study participants gave written informed consent.
2. Methods
Blood samples were collected in BD Vacutainer SST (Becton Dickinson, San Jose, CA, USA) from a median cubital vein after an overnight fasting. Chemistry tests were performed on Modular Analytics (Roche Diagnostics, Mannheim, Germany). The analytic method and the reference range in our laboratory was presented (Table 1).
3. Statistics
PASW Statistics 18 ver. 18.0.0 (SPSS Inc., Chicago, IL, USA) was used for analysis. The distribution pattern was assessed using Kolmogorov-Smirnova test. Comparisons between groups were evaluated with Mann-Whitney test and Kruskal-Wallis test. Mean values, as well as the central 90th and 95th percentile, were calculated for all measurements in each group. The significance level was set at P, 0.05.
Results
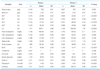
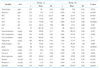
Compared with young adults (group II), elderly people (group I) showed significant increases in aspartate transaminase (AST), alanine transaminase (ALT), alkaline phosphatase (ALP), gamma-glutamyl transpeptidase (GGT), lactate dehydrogenase (LD), BUN, total cholesterol, triglyceride, and glucose, and significant decrease in high-density lipoprotein (HDL)-cholesterol (Table 2). Especially, AST, ALT, LD, total cholesterol, triglyceride, and glucose were increased with age when comparing group Ia with group Ib (Table 3). In spite of these significant differences between group I and group II, computing the central 95th percentile of group I showed that total protein, albumin, ALP, LD, creatinine, uric acid, triglyceride, HDL-cholesterol, and electrolytes were within the common reference intervals which we generally use in our laboratory. For AST and ALT, the central 90th percentile values were compatible with the common reference intervals (Figure 1). GGT, BUN, total cholesterol, low-density lipoprotein (LDL)-cholesterol, and glucose showed higher upper 97.5th and even 95th percentile values than the upper limits of the common reference intervals (Figure 2).
Discussion
Selection of an ideal reference population for the elderly people is difficult, because first, the exact definition of age for "elderly" is not clear, second, their characteristics are very heterogenous in terms of nutrition, physical activity, and medication, and third, the morbidity rates increase with age as the prevalence of cardiovascular disease, stroke, or malignancy is too high [3,6-9]. In general, "elderly" is taken to mean over 65 years of age, thus, the inclusion criterium of age in this study was 65 years or older. As an argue could be present that the subjects analyzed in this study were not representative of an healthy elderly population, authors tried to reduce the deviation by excluding those with present illness and of strong suspicion of disease from their laboratory data mentioned above. Thus there is a need to establish certain criteria to define "healthy elderly population" before conducting a future research by increasing the number of object groups in liaison with a number of laboratories.
In this study, compared with young adults, elderly people had significant increases in AST, ALT, ALP, GGT, LD, BUN, total cholesterol, triglyceride, and glucose. However, the values of most of the parameters in elderly people were similar to the common reference intervals currently used. Yet, the limitation of this study is that the 12-hour fast of the subjects was not identified in the case of triglyceride.
For most liver enzymes, the significant increases were observed in the elderly people. This finding agrees with those reported by several investigators [8,10,11]. Tietz et al. [8], however, reported higher values in 60- to 90-year-old population than younger people and then decrease after 90 years old. Fulop et al. [12] found no changes of AST. In spite of some variations, their results obtained in elderly population were in good agreement with their reference values [8,10-13]. GGT values in this study showed modest increase by age in both men and women, and were needed to be compromised.
We found an increase in glucose values with age, and this finding was also observed in other reports [8,10,14]. Although the distribution patterns of glucose values for elderly people were much higher than the usual reference intervals, the value of 97.5 percentile in elderly population was still lower than the cutoff value for a diagnosis of diabetes. As we know the high prevalence of diabetes in elderly population, a careful monitoring will be needed.
There was an increase of urea nitrogen with age. This finding agreed with most studies [6,8,14] from the aspect of decreased renal function with age. On the other hand, creatinine values showed no remarkable changes in this study, and were also very variable according to researchers [8,14]. The reason was thought that decrease in renal creatinine excretion was compensated with the low production by decreased renal mass in elderly person.
Lower albumin values in elderly people reported by other authors [8,10,12,15] suggested that it was attributed to either aging process alone or decreased state of health of these individuals. Serum iron values were also lower than those in young adults and confirmed by most [8,16,17] but not all studies.
Fraser et al. [18] brought up a question that biological variabilities should increase with age because of the compromised homeostasis, however, they confirmed that within-subject variations in elderly people were similar to those in younger subjects. Biological variations in elderly people were not investigated in this study. It was thought to be important aspect in geriatrics laboratory and needed further evaluation.
Conclusion
For routine clinical chemistry tests these results suggest that the common reference values in general are applicable to elderly people, even though some parameters showed wider distributions in elderly. However, when interpreting chemistry test results in elderly people, one should take the agerelated alterations into deep consideration. For further attempts to define the reference values for various laboratory tests in the elderly population, this study will provide a meaningful information.



 XML Download
XML Download