

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
The latissimus dorsi myocutaneous flap was one of the first methods of breast reconstruction described. However, a standard latissimus dorsi flap alone often does not provide sufficient volume for breast reconstruction and has been performed with an implant to achieve adequate breast volume. The design of an extended latissimus dorsi flap has evolved to include the parascapular and scapular fat-fascia extension in addition to lumbar fat for additional volume. The main advantage of the extended latissimus dorsi flap is that it can provide autologous tissue to the reconstructed breast without an implant and with an acceptable donor site contour and scar. The extended latissimus dorsi flap elevation is of dissection in plane just beneath the fascia superficialis, leaving the deep fat attached to the surface of the muscle. The fat left attached to the surface of the muscle is well vascularized by the perforators coming from the muscle itself. Division of the humeral attachment of the muscle is performed for an adequate excursion of the flap. Denervation of the thoracodorsal nerve is recommended for preventing postoperative involuntary muscle contraction. Patients should be warned of the potential donor site seroma. The extended latissimus dorsi flap proved to be a reliable option for totally autologous breast reconstruction in selected patients. The flap is reliable, and the procedure is technically straightforward and consistent.
Figures and Tables
Figure 1
Design for extended latissimus dorsi flap. Mark the lateral margin of the latissimus dorsi muscle along the posterior axillary line down to posterior iliac crest. The superior margin of the flap is identified by locating the tip of the scapula.

Figure 2
The planning of skin island pattern. (A) The skin island designed in the back transversely where the scar can be hidden within the confines of the bra strap. After transposition to anterior chest, skin island located inferiorly with majority of muscle located superiorly. This position helps achieve some soft tissu filling of the upper ploe of the reconstructed breast. (B) The skin island is designed laterally, obliquely in the lower midback. After transposition to anterior chest, skin island will adjacent to inframammary line. This position increases the lower pole volume and the projection of the reconstructed breast.

Figure 3
Thoracodorsal fascia dissection between superficial layer and deep layer. Dissection carried out just beneath the superficial fascia, leaving the deep fat attached to he surface of the muscle.

Figure 4
Fat-fascia extension. Extended latissimus dorsi flap has evolved to include the parascapular and scapular fat-fascia extension.

Figure 5
Flap elevation including fat-fascia extension. Superomedially, the trapezius muscle is identified and elevated away from the underlying latissimus muscle.

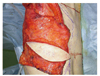
Figure 7
Pedicle dissection. Thoracodorsal artery, vein and nerve are identified at the point of entrance into muscle.

Figure 8
Flap inset. The flap transferred to the mastectomy defect through a subcutaneous tunnel high in axilla to prevent an unnatural lateral bulge and to fill the axilla.


Figure 10
Immediate breast reconstruction after modified radical mastectomy. (A) Preoperative appearance of 36-year-old woman. (B) Postoperative view after modi-fied radical mastectomy and extended latissimus dorsi flap reconstruction. (C) Postoperative view of nipple-areolar reconstruction. (D) After areolar tattoo. (E) Preoperative donor site. (F) Favorable donor site scars that will be hidden in a bra.

Figure 11
Immediate breast reconstruction after skin sparing mastectomy. (A) Preoperative appearance of 42-year-old woman. (B) Postoperative view after skin sparing mastectomy and extended latissimus dorsi flap reconstruction. (C) Postoperative view after nipple-areolar reconstruction. (D) After areolar tattoo. (E) Preoperative donor site. (F) Scar of donor site disappears over time.



References
1. Spear SL, Saba AA. Mathes SJ, Hentz VR, editors. Immediate postmastectomy recons-truction: latissimus flap techniques. Plastic surgery. 2006. Philadelphia: Saunders Elsevier;819–833.
2. Choi BC, Kim SE, Woo SH, Jeong JH, Seul JH. Immediate breast reconstruction after mastectomy for breast cancer. J Korean Soc Plast Reconstr Surg. 1997. 24:748–760.
3. Georgiade GS, Riefkohl R, Cox E, McCarty KS, Seigler HF, Georgiade NG, Snowhite JC. Long-term clinical outcome of immediate reconstruction after mastectomy. Plast Reconstr Surg. 1985. 76:415–420.

4. Robbins TH. Rectus abdominis myocutaneous flap for breast reconstruction. Aust N Z J Surg. 1979. 49:527–530.
5. Miller LB, Bostwick J 3rd, Hartrampf CR Jr, Hester TR Jr, Nahai F. The superiorly based rectus abdominis flap: predicting and enhancing its blood supply based on an anatomic and clinical study. Plast Reconstr Surg. 1988. 81:713–724.
6. Hokin JA, Silfverskiold KL. Breast reconstruction without an implant: results and complications using an extended latissimus dorsi flap. Plast Reconstr Surg. 1987. 79:58–66.
7. McCraw JB, Papp CT. Hartrampf CR, Michelow BJ, editors. Latissimus dorsi myocutaneous flap: "Fleur de Lis" reconstruction. Hartrampf's breast reconstruction with living tissue. 1991. Norfolk: Hampton Press;211–248.
8. Papp C, McCraw JB. Autogenous latissimus breast reconstruction. Clin Plast Surg. 1998. 25:261–266.
9. Germann G, Steinau HU. Breast reconstruction with the extended latissimus dorsi flap. Plast Reconstr Surg. 1996. 97:519–526.
10. Ministry of Health and Welfare. 2002 Anuual report of the Korea Central Cancer Resgistry. 2003. Seoul: Ministry of Health and Welfare.
11. Chang DW, Youssef A, Cha S, Reece GP. Autologous breast reconstruction with the extended latissimus dorsi flap. Plast Reconstr Surg. 2002. 110:751–759.
12. Moore TS, Farrell LD. Latissimus dorsi myocutaneous flap for breast reconstruction: long-term results. Plast Reconstr Surg. 1992. 89:666–672.
13. Maxwell GP. Latissimus dorsi breast reconstruction: an aesthetic assessment. Clin Plast Surg. 1981. 8:373–387.
14. Olivari N. The latissimus flap. Br J Plast Surg. 1976. 29:126–128.
15. Lee JW, Chang TW. Extended latissimus dorsi musculocutaneous flap for breast reconstruction: experience in Oriental patients. Br J Plast Surg. 1999. 52:365–372.
16. Hammond DC. Latissimus dorsi flap breast reconstruction. Plast Reconstr Surg. 2009. 124:1055–1063.
17. Ali SN, Gill P, Oikonomou D, Sterne GD. The combination of fibrin glue and quilting reduces drainage in the extended latissimus dorsi flap donor site. Plast Reconstr Surg. 2010. 125:1615–1619.
18. Dancey AL, Cheema M, Thomas SS. A prospective randomized trial of the efficacy of marginal quilting sutures and fibrin sealant in reducing the incidence of seromas in the extended latissimus dorsi donor site. Plast Reconstr Surg. 2010. 125:1309–1317.
19. Sinna R, Delay E, Garson S, Delaporte T, Toussoun G. Breast fat grafting (lipomodelling) after extended latissimus dorsi flap breast reconstruction: a preliminary report of 200 consecutive cases. J Plast Reconstr Aesthet Surg. 2010. 63:1769–1777.
20. Saint-Cyr M, Nagarkar P, Schaverien M, Dauwe P, Wong C, Rohrich RJ. The pedicled descending branch muscle-sparing latissimus dorsi flap for breast reconstruction. Plast Reconstr Surg. 2009. 123:13–24.
21. Cho HW, Lew DH, Tark KC. Effect of fibrin sealant in extended lattisimus dorsi flap donor site: retrospective study. J Korean Soc Plast Reconstr Surg. 2008. 35:267–272.
22. Delay E, Jorquera F, Lucas R, Lopez R. Sensitivity of breasts reconstructed with the autologous latissimus dorsi flap. Plast Reconstr Surg. 2000. 106:302–309.
23. Yano K, Hosokawa K, Takagi S, Nakai K, Kubo T. Breast reconstruction using the sensate latissimus dorsi musculocutaneous flap. Plast Reconstr Surg. 2002. 109:1897–1902.
 XML Download
XML Download