

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Increased number of population participating in sports results in unavoidably increase of incidence of sports injury. It also causes a rise of total healthcare expenditure. Because the technology of a variety of imaging modalities and treatment for sports injury is rapidly developed, an up-to-date knowledge on technology is critical for the sports physician. Advances in areas of nuclear medicine, magnetic resonance imaging, ultrasonography, and multi-detector computed tomography, provides a variety of options to physician in the process of patient evaluation. Therefore, they should be aware of strength, limitation, indications, contraindications, and diagnostic accuracy of diagnostic tools.
Figures and Tables
Figure 1
A patient with calcaneal stress fracture. (A) A lateral foot plain radiograph shows no definite fracture line on calcaneus.
(B)Whole body bone scintigraphy shows increased uptake at right hind foot area.

Figure 2
A patient with intra-articular calcaneal fracture. (A) A lateral foot plain radiograph shows suspicious vertical radiolucent fracture line at calcaneal body. (B) Sagittal reformatted CT image clearly shows the fracture line extending to subtalar joint. (C) Three-dimensional (3D) image with surface shaded technique (SSD) shows multiple fracture lines at a glance.

Figure 3
A patient with full-thickness tears of supraspinatus tendon. Oblique sagittal reformatted (A) and oblique coronal reformatted (B) image of shoulder CT arthrography show contrast material which injected into glenohumeral joint traverse (arrow) the supraspinatus tendon (asterisk) and reach to subacromial-subdeltoid bursa (arrowheads).
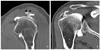
Figure 4
A patient with complete tear of extensor pollicis longus tendon (EPL) A.
Transverse sonography at the level of distal radius shows empty right third extensor compartment (arrows). B. extended field of view image shows swollen distal part of EPL which disrupted at scaphoid level.

Figure 5
US guided subacromial injection procedure. Needle tip is located between mildly thickened subdeltoid bursal wall (arrowheads).

Figure 6
A patient with transient patellar lateral subluxation. (A) Patellar skyline view of right knee shows linear increased opacity parallel to medial patellar facet (arrow) representing osteochondral fracture fragment. (B) Transaxial image of saturated proton density weighted MR image shows subchondral bone marrow contusion at medial patellar facet and lateral femoral condyle (arrows) and osteochondral fracture fragment from medial patellar facet (arrowheads).

Figure 7
A patient of medial meniscus horizontal tear. Proton density weighted coronal (A), sagittal (B), and transaxial (C) images show intrameniscal linear high signal intensity area which extend to inferior articular surface (arrows in A and B, arrowheads in C), and multilocular fluid-like high signal intensity area representing parameniscal cysts (arrow in C).

References
1. Coris EE, Zwygart K, Fletcher M, Pescasio M. Imaging in sports medicine: an overview. Sports Med Arthrosc. 2009. 17:2–12.
2. Berrington de Gonzalez A, Darby S. Risk of cancer from diagnostic X-rays: estimates for the UK and 14 other countries. Lancet. 2004. 363:345–351.

3. Orchard JW, Read JW, Anderson IJ. The use of diagnostic imaging in sports medicine. Med J Aust. 2005. 183:482–486.
4. Leffers D, Collins L. An overview of the use of bone scintigraphy in sports medicine. Sports Med Arthrosc. 2009. 17:21–24.
5. Coris EE, Higgins HW 2nd. First rib stress fractures in throwing athletes. Am J Sports Med. 2005. 33:1400–1404.
6. Humphreys SC, Eck JC, Hodges SD. Neuroimaging in low back pain. Am Fam Physician. 2002. 65:2299–2306.
7. Sanderlin BW, Raspa RF. Common stress fractures. Am Fam Physician. 2003. 68:1527–1532.
8. Lim MR, Yoon SC, Green DW. Symptomatic spondylolysis: diagnosis and treatment. Curr Opin Pediatr. 2004. 16:37–46.
9. Carek PJ, Dickerson LM, Sack JL. Diagnosis and manage-ment of osteomyelitis. Am Fam Physician. 2001. 63:2413–2420.
10. Buckwalter KA. Current concepts and advances: computerized tomography in sports medicine. Sports Med Arthrosc. 2009. 17:13–20.
11. Munshi M, Davidson M, MacDonald PB, Froese W, Sutherland K. The efficacy of magnetic resonance imaging in acute knee injuries. Clin J Sport Med. 2000. 10:34–39.
12. Megliola A, Eutropi F, Scorzelli A, Gambacorta D, De Marchi A, De Filippo M, Faletti C, Ferrari FS. Ultrasound and magnetic resonance imaging in sports-related muscle injuries. Radiol Med. 2006. 111:836–845.
13. Campbell RS, Grainger AJ. Current concepts in imaging of tendinopathy. Clin Radiol. 2001. 56:253–267.
14. Allen GM, Wilson DJ. Ultrasound in sports medicine-a critical evaluation. Eur J Radiol. 2007. 62:79–85.
15. Khan KM, Forster BB, Robinson J, et al. Are ultrasound and magnetic resonance imaging of value in assessment of Achilles tendon disorders? A two year prospective study. Br J Sports Med. 2003. 37:149–153.
16. Kijowski R, De Smet AA. The role of ultrasound in the evaluation of sports medicine injuries of the upper extremity. Clin Sports Med. 2006. 25:569–590. viii.
17. Ahn JM, El-Khoury GY. Role of magnetic resonance imaging in musculoskeletal trauma. Top Magn Reson Imaging. 2007. 18:155–168.
18. Gold GE, Hargreaves BA, Beaulieu CF. Protocols in sports magnetic resonance imaging. Top Magn Reson Imaging. 2003. 14:3–23.
 XML Download
XML Download