

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Screening mammography has been proved to be an effective tool to detect early breast cancers and to decrease mortality. However, the rate of false-negative mammograms has been reported to be still high as 10~30%. Missed breast cancers are cancers that are visible at previous mammograms only retrospectively and can be classified as three types; interval cancers, subsequent screen-detected cancers, and alternative imaging-detected cancers. In a small group, screen-detected abnormalities recalled for further evaluation may be dismissed due to false negative diagnostic assessment, leading to delays in breast cancer diagnosis. Possible causes for missing include perception errors, interpretation errors, and technical errors. Furthermore, every diagnostic examination has inherent limitations. Perception errors are often attributed to combined multiple factors; peripheral lesions, single view abnormalities, subtle findings, distracting lesions, and dense parenchyma obscuring a lesion. To decrease the false negative rate, radiologists should be alert to take additional mammograms and ultrasonography, and should try to improve the image quality and interpretation techniques comparing with the previous imaging, considering the use of computer-aided detection or double reading.
Figures and Tables
Figure 1
An interval cancer (marked by BB marker) developing 11 months after previous screening mammogram reported as negative. A small spiculated mass which was palpable seen at the time of cancer diagnosis (A) was not recognized on previous mammographic study (B). On retrospective evaluation, a tiny abnormal density was seen (B) at the periphery of left upper central breast. A lesion overlapped with pectoralis muscle caused decreased contrast.

Figure 2
An interval cancer (A) (marked by BB marker) developing 6 months after previous screening mammogram (B) reported as negative. A faint increased density is seen only on previous mediolateral oblique (MLO) view (B; right) and it is not apparent even on retrospective evaluation. However, compared with the same view from one more year prior (C), there is an interval change, suggesting of neodensity. Patient's chest wall concavity caused difficult mammographic positioning, especially in craniocaudal (CC) view.

Figure 3
An interval cancer due to underestimation of calcifications. A screening mammogram (A) showed a few punctate microcalcifications in clustered distribution (arrow), and was categorized as category 3, probably benign without taking a magnification mammogram. The Patient revisited the same hospital after 16 months and complained of palpable mass. Follow-up mammogram (B) shows increasing number and apparent pleomorphism of microcalcifications, prompting a biopsy and diagnosis of microinvasive ductal carcinoma.

Figure 4
Initial MLO (A) and craniocaudal (B) mammograms show a nonspecific parenchymal asymmetry without mass or distortion (arrows), which is attributable to physiologic asymmetry (arrow). Follow-up MLO (C) and craniocaudal (D) mammograms obtained 7 months later show slightly prominent density (arrows) and skin thickening. Histologic diagnosis was invasive ductal cancer.

Figure 5
A mammogram marked by computer-aided detection program. A circle and a rectangle mark an abnormal density and an area of microcalcifications, each.
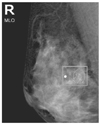
Figure 6
Subsequent screen-detected cancer. Initial bilateral craniocaudal and MLO mammograms (A) show subtle small density (arrow) at the periphery of left breast only on craniocaudal view. Subsequent screening mammograms a year later (B) clearly show an ill-defined mass (arrows).

Figure 7
Subsequent screen-detected cancer. Initial mammogram (A) show several scattered microcalcifications, attributable to benign calcifications. Subsequent screening mammograms a year later (B) show increasing fine linear calcifications in a wider area. Histologic diagnosis was low-grade ductal carcinoma in situ.

Figure 8
Alternative imaging-detected cancer. Initial bilateral craniocaudal and MLO mammograms (A) was initially interpreted as negative. Ultrasonogram taken at the same time (B) showed an irregular mass at right breast. A retrospective evaluation of mammogram show sarchitectural distortion with subtle increased density (arrow) at the corresponding site.

Figure 9
Alternative imaging-detected cancer. Annually taken right mammograms (A, B) in a patient after left mastectomy show no apparent abnormality. Chest CT (C) incidentally detected a mass at medial portion of right breast (arrow). After verification of abnormal mass with targeted ultrasound (D), a retrospective evaluation of mammograms (B) showed a subtle increased density (dotted arrow) at right upper posterior breast, which was denser than previous mammographic evaluation (A).
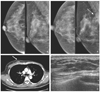
Figure 10
Alternative imaging-detected cancer. Mammograms (A) in a patient with metastatic lymph node at right axilla show no apparent abnormality in breast. Breast magnetic resonance imaging before (left) and after (right) contrast administration (B) detected an enhancing mass (arrow). After verification of abnormal mass with targeted ultrasound (C), a retrospective evaluation of mammograms (A) showed a tiny mass (dotted arrow) at right upper posterior breast, which was histologically diagnosed as invasive ductal cancer.

Figure 11
Recalled but dismissed cancer. Right unilateral mammograms (A) in a patient after left mastectomy showed an abnormal density (arrow) only seen on MLO view. Problem solving breast ultrasonographic evaluation did not detect any suspicious lesion. A captured sonogram of right upper outer quadrant (B; left) show normal fibroglandular tissue and a captured image of right upper inner quadrant (B; right) show a benign-appearing mass (B), which cannot be accounted for mammographic density. On magnification mammogram (C), which was taken 6 months later an ill-defined mass is clearly seen. Re-evaluation sonographic evaluation (D) identified a 1.5 cm sized malignant mass at right middle outer portion, 9 o'clock position.

Figure 12
Recalled but dismissed cancer. Initial mammogram (A) shows subtle microcalcifications (arrows) in a whole upper outer quadrant, which were poorly defined due to poor compression and contrast. Initial sonogram of the same quadrant (B) shows a normal appearing fibroglandular tissue. Six months follow-up mammogram (C) shows pleomorphic microcalcifications (arrows), better seen with improved compression and exposure. Follow-up sonogram of the same site (D) shows multiple microcalcifications (arrows), which was confirmed as ductal carcinoma in situ.


References
1. Fletcher SW, Black W, Harris RP, Rimer BK, Shapiro S. Report of the International Workshop on Screening for Breast Cancer. J Natl Cancer Inst. 1993. 85:1644–1656.

2. Harris R, Leininger L. Clinical strategies for breast cancer screening: weighing and using the evidence. Ann Intern Med. 1995. 112:539–547.
3. Kerlikowske K, Grady D, Rubin S, Sandrock C, Ernster VL. Efficacy of screening mammography. A meta-analysis. JAMA. 1995. 273:149–154.
4. Tabár L, Fagerberg CJ, Gad A, Baldetorp L, Holmberg LH, Gröntoft O, Ljungquist U, Lundström B, Månson JC, Eklund G. Reduction in mortality from breast cancer after mass screening with mammography. Randomised trial from the Breast Cancer Screening Working Group of the Swedish National Board of Health and Welfare. Lancet. 1985. 1:829–832.
5. Houssami N, Irwig L, Ciatto S. Radiological surveillance of interval breast cancers in screening programmes. Lancet Oncol. 2006. 7:259–265.
6. Warren RM, Young JR, McLean L, Lyons K, Wilson AR, Evans A, Duffy SW, Warsi IM. Radiology review of the UKCCCR Breast Screening Frequency Trial: potential improvements in sensitivity and lead time of radiological signs. Clin Radiol. 2003. 58:128–132.
7. Harvey JA, Fajardo LL, Innis CA. Preview mammograms on patients with impalpable breast carcinoma: Retrospective vs blind interpretation. AJR Am J Roentgenol. 1993. 161:1167–1172.
8. Warren R, Duffy S. Interval cancers as an indicator of performance in breast screening. Breast Cancer. 2000. 7:9–18.
9. Buist DS, Porter PL, Lehnman C, Taplin SH, White E. Factors contributing to mammography failure in women aged 40-49 years. J Natl Cancer Inst. 2004. 96:1432–1440.
10. Brenner RJ. False-negative mammograms. Medical, legal, and risk management implications. Radiol Clin North Am. 2000. 38:741–757.
11. Han BK, Kim JY, Shin JH, Choi YH. Performance of computer-aided detection in false negative screening mammograms of breast cancers. J Korean Radiol Soc. 2004. 51:465–472.
12. Soo MS, Baker JA, Rosen EL. Sonographic detection and sonographically guided biopsy of breast microcalcifications. AJR Am J Roentgenol. 2003. 180:941–948.
13. Majid AS, de Paredes ES, Doherty RD, Sharma NR, Salvador X. Missed Breast Carcinoma: Pitfalls and Pearls. Radiographics. 2003. 23:881–895.
 XML Download
XML Download