

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
In all clinical trials comparing rate versus rhythm control of atrial fibrillation (AF) by drugs, there was no survival benefit associated with a rhythm control strategy. Currently used antiarrhythmic drugs are not only frequently ineffective at eliminating AF, but may be life threatening in some patients. Catheter ablation (CA) of AF has evolved rapidly and has become accepted as one of the therapeutic modalities for controlling AF. The effective strategies for CA of AF consist of pulmonary vein isolation (PVI) and/or complete encirclement around PVs with or without additional ablation lines. Selection of patients, who may be benefited by CA or not, is an important issue. Precise electroanatomic mapping for the triggers and the substrate of the atria is central for customizing ablation target and for enhancing efficacy of CA for AF. With further development of new energy sources of ablation, cardiac imaging, navigation, and mapping systems, the CA can be simplified and standardized, which may enable the CA to become more effective, safer, and more applicable to many different subsets of AF.
Figures and Tables
Figure 1
Selection of antiarrhythmic drugs for the maintenance of sinus rhythm. ACC/AHA/ESC Practice Guidelines 2006.


Figure 3
Number of catheter ablation of atrial fibrillation at Korea University Medical Center (KUMC, 1998~2007, n=680).
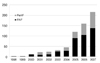
Figure 4
Long-term freedom from AF recurrence in patients with paroxysmal AF and persistent AF at KUMC (n=533).
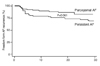
Figure 5
Selective arrhythmogenic pulmonary vein isolation (A) and empirical 4 pulmonary veins isolation (B). Pak HN, et al. J Cardiovasc Electrophysiol 2008 (In press).

Figure 6
Atrial fibrillation recurrence rate after selective arrhythmogenic pulmonary vein isolation (SePVI) and empirical 4 pulmonary veins isolation (EmPVI). Pak HN, et al. J Cardiovasc Electrophysiol 2008 (In press).

Figure 7
Automated map of complex fractionated atrial electrograms (CFAEs) during atrial fibrillation (6 seconds segment). The areas of white and red color illustrate CFAE with cycle length <80ms and <120ms, respectively.

Figure 8
Linear ablation along the complex fractionated atrial electrograms (CFAEs, white color denotes cycle length <120ms) during atrial fibrillation. Panel A shows automated CFAE map at baseline and panel B shows the summary of ablation of the antra of 4 pulmonary veins and linear extension to the areas showing CFAE.


References
1. Wyse DG, Waldo AL, DiMarco JP, Domanski MJ, Rosenberg Y, Schron EB, Kellen JC, Greene HL, Mickel MC, Dalquist JE, Corley SD. Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM). Investigators. A comparison of rate control and rhythm control in patients with atrial fibrillation. N Engl J Med. 2002. 347:1825–1833.

2. Haïssaguerre M, Jaïs P, Shah DC, Takahashi A, Hocini M, Quiniou G, Garrigue S, Le Mouroux A, Le Métayer P, Clémenty J. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med. 1998. 339:659–666.
3. Pak HN, Hwang C, Lim HE, Kim JW, Lee HS, Kim YH. Electroanatomic characteristics of atrial premature beats triggering atrial fibrillation in patients with persistent versus paroxysmal atrial fibrillation. J Cardiovasc Electrophysiol. 2006. 17:818–824.
4. Rha SW, Kim YH, Hong MK, Ro YM, Choi CU, Suh SY, Kim JW, Kim EJ, Park CG, Seo HS, Oh DJ. Mechanisms responsible for the initiation and maintenance of atrial fibrillation assessed by non-contact mapping system. Int J Cardiol. 2008. 124:218–226.
5. Haïssaguerre M, Jaïs P, Shah DC, Garrigue S, Takahashi A, Lavergne T, Hocini M, Peng JT, Roudaut R, Clémenty J. Electrophysiological end point for catheter ablation of atrial fibrillation initiated from multiple pulmonary venous foci. Circulation. 2000. 101:1409–1417.
6. Marrouche NF, Dresing T, Cole C, Bash D, Saad E, Balaban K, Pavia SV, Schweikert R, Saliba W, Abdul-Karim A, Pisano E, Fanelli R, Tchou P, Natale A. Circular mapping and ablation of the pulmonary vein for treatment of atrial fibrillation: impact of different catheter technologies. J Am Coll Cardiol. 2002. 40:464–474.
7. Oral H, Knight BP, Tada H, Ozaydin M, Chugh A, Hassan S, Scharf C, Lai SW, Greenstein R, Pelosi F Jr, Strickberger SA, Morady F. Pulmonary vein isolation for paroxysmal and persistent atrial fibrillation. Circulation. 2002. 105:1077–1081.
8. Pappone C, Oreto G, Rosanio S, Vicedomini G, Tocchi M, Gugliotta F, Salvati A, Dicandia C, Calabrò MP, Mazzone P, Ficarra E, Di Gioia C, Gulletta S, Nardi S, Santinelli V, Benussi S, Alfieri O. Atrial electroanatomic remodeling after circumferential radiofrequency pulmonary vein ablation: efficacy of an anatomic approach in a large cohort of patients with atrial fibrillation. Circulation. 2001. 104:2539–2544.
9. Oral H, Scharf C, Chugh A, Hall B, Cheung P, Good E, Veerareddy S, Pelosi F Jr, Morady F. Catheter ablation for paroxysmal atrial fibrillation: segmental pulmonary vein ostial ablation versus left atrial ablation. Circulation. 2003. 108:2355–2360.
10. Kottkamp H, Tanner H, Kobza R, Schirdewahn P, Dorszewski A, Gerds-Li JH, Carbucicchio C, Piorkowski C, Hindricks G. Time courses and quantitative analysis of atrial fibrillation episode number and duration after circular plus linear left atrial lesions: trigger elimination or substrate modification: early or delayed cure? J Am Coll Cardiol. 2004. 44:869–877.
11. Vasamreddy CR, Dalal D, Eldadah Z, Dickfeld T, Jayam VK, Henrickson C, Meininger G, Dong J, Lickfett L, Berger R, Calkins H. Safety and efficacy of circumferential pulmonary vein catheter ablation of atrial fibrillation. Heart Rhythm. 2005. 2:42–48.
12. Ouyang F, Bänsch D, Ernst S, Schaumann A, Hachiya H, Chen M, Chun J, Falk P, Khanedani A, Antz M, Kuck KH. Complete isolation of left atrium surrounding the pulmonary veins: new insights from the double-Lasso technique in paroxysmal atrial fibrillation. Circulation. 2004. 110:2090–2096.
13. Pak HN, Kim JS, Shin SY, Lee HS, Choi JI, Lim HE, Hwang C, Kim YH. Is Empirical Four Pulmonary Vein Isolation Necessary for Focally Triggered Paroxysmal Atrial Fibrillation? Comparison of Selective Pulmonary Vein Isolation Versus Empirical Four Pulmonary Vein Isolation. J Cardiovasc Electrophysiol. 2008. 02. 12. [Epub ahead of print].
14. Nademanee K, McKenzie J, Kosar E, Schwab M, Sunsaneewitayakul B, Vasavakul T, Khunnawat C, Ngarmukos T. A new approach for catheter ablation of atrial fibrillation: mapping of the electrophysiologic substrate. J Am Coll Cardiol. 2004. 43:2044–2053.
15. Oral H, Chugh A, Good E, Wimmer A, Dey S, Gadeela N, Sankaran S, Crawford T, Sarrazin JF, Kuhne M, Chalfoun N, Wells D, Frederick M, Fortino J, Benloucif-Moore S, Jongnarangsin K, Pelosi F Jr, Bogun F, Morady F. Radiofrequency catheter ablation of chronic atrial fibrillation guided by complex electrograms. Circulation. 2007. 115:2606–2612.
16. Scherlag BJ, Yamanashi WS, Schauerte P, Scherlag M, Sun YX, Hou Y, Jackman WM, Lazzara R. Endovascular stimulation within the left pulmonary artery to induce slowing of heart rate and paroxysmal atrial fibrillation. Cardiovasc Res. 2002. 54:470–475.
17. Oh S, Zhang Y, Bibevski S, Marrouche NF, Natale A, Mazgalev TN. Vagal denervation and atrial fibrillation inducibility: epicardial fat pad ablation does not have long-term effects. Heart Rhythm. 2006. 3:701–708.
18. Bertaglia E, Zoppo F, Tondo C, Colella A, Mantovan R, Senatore G, Bottoni N, Carreras G, Corò L, Turco P, Mantica M, Stabile G. Early complications of pulmonary vein catheter ablation for atrial fibrillation: a multicenter prospective registry on procedural safety. Heart Rhythm. 2007. 4:1265–1271.
19. Kim JH, Shin SY, Joo HJ, Hong SJ, Lim HE, Choi JI, Pak HN, Kim YH. Drug-eluting stent for the therapy of pulmonary vein stenosis developed after catheter ablation of atrial fibrillation. Korean Circ J. 2008. (in press).
20. Wazni OM, Marrouche NF, Martin DO, Verma A, Bhargava M, Saliba W, Bash D, Schweikert R, Brachmann J, Gunther J, Gutleben K, Pisano E, Potenza D, Fanelli R, Raviele A, Themistoclakis S, Rossillo A, Bonso A, Natale A. Radiofrequency ablation vs antiarrhythmic drugs as first-line treatment of symptomatic atrial fibrillation: a randomized trial. JAMA. 2005. 293:2634–2640.
21. Hsu LF, Jaïs P, Sanders P, Garrigue S, Hocini M, Sacher F, Takahashi Y, Rotter M, Pasquié JL, Scavée C, Bordachar P, Clémenty J, Haïssaguerre M. Catheter ablation for atrial fibrillation in congestive heart failure. N Engl J Med. 2004. 351:2373–2383.
 XML Download
XML Download