

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Patients with community-acquired pneumonia can be divided into four groups, each with a list of likely pathogens and suggested empiric therapy accordingly. Patient classification is based on the assessment of place of therapy, the presence of cardiopulmonary disease, and the presence of modifying factors. The admission decision remains to be difficult and follows the prognostic scoring rules (the Pneumonia Patients Outcome Research Team, PORT) are widely using as admission criteria. Still clinicians use inconsistent admission criteria and often overestimate patients risk. In general, hospitalization is needed if patients have multiple risk factors for a complicated course. Admission to the intensive care unit is needed for patients with severe community-acquired pneumonia.
Figures and Tables

Figure 2
Severity assessment in a hospital setting: the CURB-65 score. One step strategy for stratifying patients with community-acquired pneumonia risk groups according to risk of mortality at 30 days when the results of blood urea are available.
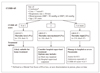
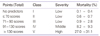
Table 1
Four patients groups according to American Thoracic Society community-acquired pneumonia guidelines








References
1. Niederman MS, Mandell LA, Anzueto A, Bass JB, Broughton WA, Campbell GD, Dean N, File T, Fine MJ, Gross PA, Martinez F, Marrie TJ, Plouffe JF, Ramirez J, Sarosi GA, Torres A, Wilson R, Yu VL. American Thoracic Society. Guidelines for the management of adults with community-acquired pneumonia. Diagnosis, assessment of severity, antimicrobial therapy, and prevention. Am J Respir Crit Care Med. 2001. 163:1730–1754.

2. Fine MJ, Orloff JJ, Arisumi D, Fang GD, Arena VC, Hanusa BH, Yu VL, Singer DE, Kapoor WN. Prognosis of patients hospitalized with community-acquired pneumonia. Am J Med. 1990. 88:1N–8N.
3. Fine MJ, Smith DN, Singer DE. Hospitalization decision in patients with community-acquired pneumonia: a prospective cohort study. Am J Med. 1990. 89:713–721.
4. The aetiology, management and outcome of severe community-acquired pneumonia on the intensive care unit. The British Thoracic Society Research Committee and The Public Health Laboratory Service. Respir Med. 1992. 86:7–13.
5. Mandell LA, Marrie TJ, Grossman RF, Chow AW, Hyland RH. Canadian guidelines for the initial management of community-acquired pneumonia: an evidence-based update by the Canadian Infectious Diseases Society and the Canadian Thoracic Society. The Canadian Community-Acquired Pneumonia Working Group. Clin Infect Dis. 2000. 31:383–421.
6. Mandell LA, Bartlett JG, Dowell SF, File TM Jr, Musher DM, Whitney C. Update of practice guidelines for the management of community-acquired pneumonia in immunocompetent adults. Clin Infect Dis. 2003. 37:1405–1433.
7. Fine MJ, Smith MA, Carson CA, Mutha SS, Sankey SS, Weissfeld LA, Kapoor WN. Prognosis and outcomes of patients with community-acquired pneumonia. A meta-analysis. JAMA. 1996. 275:134–141.
8. Fine MJ, Auble TE, Yealy DM, Hanusa BH, Weissfeld LA, Singer DE, Coley CM, Marrie TJ, Kapoor WN. A prediction rule to identify low-risk patients with community-acquired pneumonia. N Engl J Med. 1997. 336:243–250.
9. Marrie TJ, Huang JQ. Low-risk patients admitted with community-acquired pneumonia. Am J Med. 2005. 118:1357–1363.
10. Ruiz M, Ewig S, Torres A, Arancibia F, Marco F, Mensa J, Sanchez M, Martinez JA. Severe community-acquired pneumonia. Risk factors and follow-up epidemiology. Am J Respir Crit Care Med. 1999. 160:923–929.
11. Torres A, Serra-Batlles J, Ferrer A, Jiménez P, Celis R, Cobo E, Rodriguez-Roisin R. Severe community-acquired pneumonia. Epidemiology and prognostic factors. Am Rev Respir Dis. 1991. 144:312–318.
12. McMahon LF Jr, Wolfe RA, Tedeschi PJ. Variation in hospital admissions among small areas. A comparison of Maine and Michigan. Med Care. 1989. 27:623–631.
13. Roos NP, Wennberg JE, McPherson K. Using diagnosis-related groups for studying variations in hospital admissions. Health Care Financ Rev. 1988. 9:53–62.
14. Wennberg JE, Freeman JL, Culp WJ. Are hospital services rationed in New Haven or over-utilized in Boston? Lancet. 1987. 1:1185–1189.
15. Fine MJ, Hough LJ, Medsger AR, Li YH, Ricci EM, Singer DE, Marrie TJ, Coley CM, Walsh MB, Karpf M, Lahive KC, Kapoor WN. The hospital admission decision for patients with community-acquired pneumonia. Results from the pneumonia Patient Outcomes Research Team cohort study. Arch Intern Med. 1997. 157:36–44.
16. Auble TE, Yealy DM, J MJ. Commutity-acquired pneumonia in adults: Risk stratification and the decision to admit. 2007. 2007 UpToDate.
17. Lim WS, van der Eerden MM, Laing R, Boersma WG, Karalus N, Town GI, Lewis SA, Macfarlane JT. Defining community acquired pneumonia severity on presentation to hospital: an international derivation and validation study. Thorax. 2003. 58:377–382.
18. Lim WS, Macfarlane JT, Boswell TC, Harrison TG, Rose D, Leinonen M, Saikku P. Study of community acquired pneumonia aetiology (SCAPA) in adults admitted to hospital: implications for management guidelines. Thorax. 2001. 56:296–301.
19. Bauer TT, Ewig S, Marre R, Suttorp N, Welte T. CRB-65 predicts death from community-acquired pneumonia. J Intern Med. 2006. 260:93–101.
20. Aujesky D, Auble TE, Yealy DM, Stone RA, Obrosky DS, Meehan TP, Graff LG, Fine JM, Fine MJ. Prospective comparison of three validated prediction rules for prognosis in community-acquired pneumonia. Am J Med. 2005. 118:384–392.
 XML Download
XML Download