

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
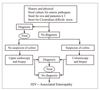
There are various diagnostic methods for detection of HIV infection. Among them, ELISA has been using most widely as a screening test. On the other hand, the Western blot method has been used as a confirmative test. The final confirmative tests are conducted on the seropositive sample and other supplementary methods such as HIV antigen test or molecular tests involving polymerase chain reaction should be performed in addition to Western blot for the confirmation. The clinical consequences of HIV infection encompass a spectrum ranging from an acute syndrome associated with primary infection to a prolonged asymptomatic state and advanced disease. It is best to regard HIV disease as beginning at the time of primary infection and progressing through various stages. Throughout the course of HIV infection, active viral replication and progressive immunologic impairment occur in most patients. With the exception of rare true long-term nonprogressors, HIV disease, when untreated, inexorably progresses even during the clinically latent stage. However, anti-retroviral therapy has had a major impact on blocking or slowing the progression of disease over extended periods of time in a substantial proportion of adequately treated patients. Overall, the clinical spectrum of HIV disease is constantly changing as patients live longer and new and better approaches to treatment and prophylaxis are developed.
Figures and Tables




References
1. Kim JM, Cho GJ, Hong SK, Chang KH, Chung JS, Choi YH, Song YG, Huh AJ, Yeom JS, Lee KS, Choi JY. Epidemiology and Clinical Features of HIV Infection/AIDS in Korea. Yonsei Med J. 2003. 44:363–370.

2. CDC. 1993 Revised classification system for HIV infection and expanded surveillance case definition for AIDS among adolescents and adults. MMWR. 1992. 41:1–19.
3. CDC. Surveillance for AIDS-defining opportunistic illness, 1992-1997. MMWR. 1999. 48:1–22.
4. Grant AD, Djomand G, De Cock KM. Natural history and spectrum of disease in adults with HIV/AIDS in africa. AIDS. 1997. 11:S43–S54.
5. Klein RS, Harris CA, Small CB, Moll B, Lesser M, Friedland GH. Oral candidiasis in high-risk patients as the initial manifestation of the acquired immunodeficiency syndrome. N Engl J Med. 1984. 311:354–358.
6. Mandell GL, Bennett JE, Dolin R. Principles and Practice of Infectious Diseases. 2000. 5th ed. Philadelphia: Churchill Livingstone;1404–1409.
7. Munoz A, Schroger L, Bacellar H, Speizer I, Vermund SH, Detels R, Saah AJ, Kingslev LA, Seminara D, Phair JP. Trends in the incidence of outcomes defining acquired immunodeficiency syndrome(AIDS) in the multicenter AIDS study, 1985-1991. Am J Epidemiol. 1993. 137:423–438.
8. Sansone GR, Frengley JD. Impact of HAART on cause of death of persons with late-stage AIDS. J Urban Health. 2000. 77:166–175.
 XML Download
XML Download