

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Multidetector computed tomography (MDCT) has been developed for the purpose of reducing the scan time and enlarging the scan coverage. In benefit of multiple arrays of detectors along with faster gantry, MDCT has now become an inevitable diagnostic tool for various kinds of musculoskeletal diseases. Three-dimensional reconstruction images are the basic method in all kinds of musculoskeletal images. Multiplanar reformat, surface rendering, and maximum intensity projections are frequently used techniques. Occult fractures in complex anatomic regions, joint disease evaluations including internal derangement of the joints, and cartilage lesions can be assessed accurately with MDCT. Indirect intravenous contrast enhanced angiographic images are much improved from the previous version of CT or MRI in terms of differentiating individual phases of contrast filling. MDCT is a 3D-oriented diagnostic tool, and one must acknowledge appropriate scan parameters in order to obtain the best 3D results. MDCT is one of the hottest imaging tool in the field of diagnostic radiology. Sixty-four detector CT is now popular, and 512 and more advanced detectors such as 2-dimensional fat panel CT are expected to appear in the near future. A thorough knowledge on the application of MDCT is necessary in order to use this state-of-the-art imaging equipment efficiently in our daily practice.
Figures and Tables
 | Figure 1Arrangement of detectors of multidetector computed tomography machine of major vendors. The diagram on the left is four slice scanners, and on the right is 16 slice scanner. Minimum 0.625 mm sized detector elements are used in the center of the array
|
 | Figure 2Types of three dimensional reconstruction
(A) Multiplanar reformat image of mandible reformatted along the curve of axis of mandible. Like panorama view, all mandiblular structures are displayed in one plane
(B) Surface rendering image of acetabular fracture. Fracture fragements are visualized efficiently with this technique
(C) Maximum intensity projection image of ankle fracture. Evaluation of fracture anatomy is more easy with this view
|
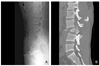 | Figure 3(A) Fracture dislocation is noted in midlumbar spine. Fragment is not clearly seen in plain radiography
(B) Sagittal reformat image of the same patient shows posterior displacement of fracture fragment into the spinal canal
|
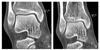
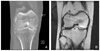 | Figure 4(A) CT arthrographic image of the knee. Cartilage surface is clearly identified
(B) MR image of same patient show metallic artifact due to surgical materials
|

References
1. Ohashi K, El-Khoury GY, Abu-Zahra KW. Interobserver Agreement for Letournel Acetabular Fracture Classification with Multidetector CT: Are Standard Judet Radiographs Necessary? Radiology. 2006. 241:386–391.

2. Memarsadeghi M, Breitenseher MJ, Schaefer-Prokop C, Weber M, Aldrian S, Gabler C, Prokop M. Occult Scaphoid Fractures: Comparison of Multidetector CT and MR Imaging-Initial Experience. Radiology. 2006. 240:169–176.
3. Waldt S, Bruegel M, Ganter K, Kuhn V, Link TM, Rummeny EJ, Woertler K. Comparison of multislice CT arthrography and MR arthrography for the detection of articular cartilage lesions of the elbow. Eur Radiol. 2005. 15:784–791.
4. Mutschler C, Vande Bera BC, Lecouvet FE, Poilvache P, Dubuc JE, Maldague B, Malghem J. Postoperative meniscus: assessment at dual-detector row spiral CT arthrography of the knee. Radiology. 2003. 228:635–641.
5. Vande Berg BC, Lecouvet FE, Poilvache P, Dubuc JE, Maldague B, Malghem J. Anterior cruciate ligament tears and associated meniscal lesions: assessment at dual-detector spiral CT arthrography. Radiology. 2002. 223:403–409.
6. Rand T, Brossmann J, Pedowitz R, Ahn JM, Haghigi P, Resnick D. Analysis of patellar cartilage. Comparison of conventional MR imaging and MR and CT arthrography in cadavers. Acta Radiol. 2000. 41:492–497.
7. El-Khoury GY, Alliman KJ, Lundberg HJ, Rudert MJ, Brown TD, Saltzman CL. Cartilage thickness in cadaveric ankles: measurement with double-contrast multi-detector row CT arthrography versus MR imaging. Radiology. 2004. 233:768–773.
8. Schmid MR, Pfirrmann CW, Hodler J, Vienne P, Zanetti M. Cartilage lesions in the ankle joint: comparison of MR arthrography and CT arthrography. Skeletal Radiol. 2003. 32:259–265.
9. Vande Berg BC, Lecouvet FE, Poilvache P, Jamart J, Materne R, Lengele B, Maldague B, Malghem J. Assessment of knee cartilage in cadavers with dual-detector spiral CT arthrography and MR imaging. Radiology. 2002. 222:430–436.
10. Sunagawa T, Ochi M, Ishida O, Ono C, Ikuta Y. Threedimensional CT imaging of flexor tendon ruptures in the hand and wrist. J Comput Assist Tomogr. 2003. 27:169–174.
11. Nakamae A, Deie M, Yasumoto M, Adachi N, Kobayashi K, Yasunaga Y, Ochi M. Three-Dimensional Computed Tomography Imaging Evidence of Regeneration of the Semitendinosus Tendon Harvested for Anterior Cruciate Ligament Reconstruction: A Comparison With Hamstring Muscle Strength. J Comput Assist Tomogr. 2005. 29:241–245.
12. Abdelmoumene Y, Chevallier P, Barghouth G, Protier F, Qanadli SD, Doenz F, Schnycler P, Denys A. Optimization of Multidetector CT Venography Performed with Elastic Stockings on Patient's Lower Extremities: A Preliminary Study of Nonthrombosed Veins. Am J Roentgenology. 2003. 180:1093–1094.
 XML Download
XML Download