

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Repairing non-union fractures or bony defects is surgically challenging. Synthetic bone substitutes and osteogenic materials have been evaluated as aids [2,18,29,31]. Among the synthetic bone substitutes, hydroxyapatite and other calcium phosphate ceramics have shown the most promising results due to their osteoconductive properties, unlimited availability and absence of immune response [9,25,28]. A potential limitation of such materials is the slow biodegradation rate observed in pure hydroxyapatite. However, implants comprised of beta-tricalcium phosphate (β-TCP) are resorbable [6]. β-TCP has shown good biocompatibility and osseointegration, but appreciable amounts were still present after 12 months [17].
Recently, it has been reported that umbilical cord blood can serve as an alternative source of mesenchymal stem cells (MSCs), and human umbilical cord blood-derived MSCs (UCB-MSCs) contain multi-potent cells including those with osteogenic potential [22,27]. Furthermore, UCB-MSCs may be immune-privileged cells with surface characteristics that enable circumvention of immune rejection [5,7]. Recently, we isolated canine UCB-MSCs [21], which provides a ready source of the cells.
The present study reports enhanced osteogenesis by the implantation of canine UCB-MSCs mixed with β-TCP in bone defect model dogs, and the successful repair of a non-union fracture case by allografting and injection of canine UCB-MSCs.
Materials and Methods
Animals
Six healthy Beagle dogs (15.4 ± 1.2 months, B.W 6~7 kg) were used for the orthotopic implantation. There were two experimental groups: canine UCB-MSCs grafting and control, with three dogs per group. The dogs were housed in indoor cages. Food and water were supplied ad libitum. All animal experiments conformed to the Guidelines for Animal Experiments of Seoul National University.
Preparation of canine UCB-MSCs
Fetal umbilical cord blood was collected during Caesarean section of pregnant female dogs. Canine UCB-MSCs were produced by culturing to facilitate proliferation of mononucleated cells from cord blood as verified by fluorescence-activated cell sorting (FACS) analysis, and by the in vitro differentiation of bone [21]. Cells (1 × 106) were prepared for implantation. Canine UCB-MSCs were suspended with 500 µl of normal saline prior to mixing with 700 mg of β-TCP (group CM). The same volume of normal saline mixed with β-TCP was prepared as the control (group C).
Bioceramic implants
β-TCP powder and the β-TCP/poly L-lactide-co-ε-caprolactone composite (TCP/PLGC) membrane were gifts of the Biomaterials Center, National Institute for Materials Science, Japan. β-TCP particle diameter averaged about 125 µm and the molecular weight of PLGC was 250,000. Each TCP/PLGC membrane was prepared by mixing β-TCP particles and PLGC in a weight ratio of 7:3 for 10 min at 180℃. The composite was formed into 200 µm thick membranes with a hot-press [15].
Orthotopic implantation and harvest
After dogs were premedicated with 0.2 mg butorphanol (Myungmoon Pharm, Korea) at a dose of 0.2 mg/kg body weight and acepromazine maleate (Samwoo, Korea) at a dose of 0.05 mg/kg body weight, 1% propofol (Claris Lifesciences, India) at a dose of 6 mg/kg body weight was intravenously injected to induce anesthesia. Isoflurane (Ilsung Pharmaceutical, Korea) was used to maintain anesthesia. Under sterile conditions, a craniomedial approach was performed to expose the diaphysis of right radius. The periosteum was elevated only enough to allow the plate to lie directly on the bone. An eight-hole, 2.7 dynamic compression plate (Synthes, Switzerland) was contoured and applied to the cranial aspect of the radius. The plate was then removed and a 15 mm long osteoperiosteal segmental cortical defect was made at the mid-portion of the diaphysis with an oscillation bone saw [3]. The plate was then reapplied, mixed materials were implanted in the defect, and the implanted site was wrapped with TCP/PLGC to prevent leakage of implants. After closing the soft tissue, a Robert John's bandage was applied for 2 weeks. The implants were harvested 12 weeks after implantation.
Radiographic examination
Lateral and craniocaudal radiographs of the right antebrachium were made before and immediately after surgery as well as 2, 4, 8 and 12 weeks after implantation. Each radiographic evaluation focused on the continuity between host bone and implant, and the change of implant radiopacity.
Histological examination
Segments of bone including defect sites were removed and processed for histological analysis without decalcification. Specimens were fixed in 4% paraformaldehyde and processed for methyl methacrylate embedding using an Osteo-Bed Bone embedding kit (Polysciences, USA). Longitudinal sections were cut in the sagittal planes using a microtome. The central longitudinal sections from each radius were ground to a thickness of 100 µm and stained with hematoxylin and eosin (H&E), toluidine blue, and Villanueva-Goldner stains to evaluate new bone formation. Stained sections from each group were observed under a light microscope and were scanned using an attached digital camera and a NIS-Elements system (Nikon, Japan). The areas of new bone formation and the residual β-TCP were determined and converted to a percentage of total area of bone defect.
Statistics
Student's t-test was performed to compare the new bone formation between the C and CM groups at a 95% confidence level.
Clinical application
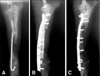
A 6-month-old Toy poodle that had been operated on twice previously presented to the Veterinary Medical Teaching Hospital, Seoul National University, with radial non-union fracture (Fig. 1A). A cortical allograft was implanted (Fig. 1B). Graft lysis and instability of fractured site were observed 9 weeks after implantation (Fig. 1C). Under fluoroscopy-aided guidance, 1 × 107 canine UCB- MSCs diluted with 0.5 ml saline were injected into the bone defect formed by graft lysis. Another injection was done 1 month later.
Results
Animal model
All dogs were able to bear weight partially by 2 weeks, after which they became active in their enclosures. All wounds healed without infection and there were no failures of fixation.
Radiographic findings
Postoperatively, the defect could be visualized easily because of the radiopacity of the material. With time, the radiolucent site gradually expanded from interface between the host bone and the implant to the central part of the defect in both groups, but the tendency was clearer in group CM (Fig. 2). Radiolucency was found only near the bone end in group C by 12 weeks but was evident throughout the entire graft in group CM.
Histological findings
Bone formation was observed around β-TCP in longitudinal sections of implants in both groups 12 weeks after implantation (Fig. 3). β-TCP remained in both sides and the distal one third of the implant, especially under the fixation plate and in group C. Osteocytes were evident around the β-TCP (Fig. 4A). New bone was in direct contact with the β-TCP granules (Figs. 4B and C). Histomorphometric analysis revealed percentages of new bone formation in groups C and CM were 4.08 ± 2.08 and 10.92 ± 2.74, respectively (p < 0.05). Residual percentages of β-TCP were 40.63 ± 17.86 and 24.21 ± 8.75, in groups C and CM, respectively (Table 1).
Clinical application
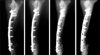
Radiographically, increased opacity between radius and allograft bone, and a decreased radiolucent gap was checked four weeks after injection of canine UCB-MSCs. With time, the radiolucent site gradually decreased and the radiolucent fracture line disappeared (Fig. 5). Instability at fracture site was decreased by 8 weeks after injection. The dog could bear weight partially by 8 weeks.
Discussion
Radiography is useful to assess the union at host bone-implant interfaces as an important factor of bone healing [1,3]. Presently, a distinct radiolucent zone at the interface between implants and the host bone was visible on the immediate postoperative radiographs. The absence of this radiolucent zone was considered to be an indication of union between the implant and the host bone. In the present study, union at the host bone-implant interface occurred more often and more rapidly in group CM than group C. An ideal bone graft substitute should resorb fully and at a predictable rate, while also providing a three-dimensional matrix to support bone ingrowth and ongrowth during resorption [33]. The appearance of implanted β-TCP on X-rays was the density of bone in early phase. Thereafter, as further resorption of the β-TCP and bone remodeling occurred, density decreased more [32]. In this study, radiolucency was found only near the bone end in group C, but throughout the entire graft in group CM at 12 weeks.
Previous studies used bloc ceramics with pores precultured with cells in osteogenic medium or vacuumed for uniform loading and retention of cells [13,34]. In the present study, β-TCP granules were mixed with cells immediately before implantation; this method of cell-matrix combination can be easily performed in a clinical setting.
In the previous report [3], new bone was distributed uniformly throughout the cell-matrix implant. However, in the present study, β-TCP remained in both sides and the distal one third of the implant, especially under the fixation plate and in group C, as evident histologically 12 weeks after implantation. β-TCP that remained under the fixation plate could be due to impaired blood supply to outer cortical bone beneath plates [8]. In the present study, implants were wrapped with TCP/PLGC membrane to prevent leakage of the β-TCP granule-cell mixture and invasion of fibrous connective tissues into the implant instead of vascular and host bone ingrowth. In assessing the present observations, it was suggested that vascular or bone ingrowth may have depended largely on proximal host bone. Bone formation with bone graft substitute relies on a complex sequence of events with a major dependence on vascular ingrowth, differentiation of osteoprogenitor cells, bone remodeling and graft resorption that occur together with host bone ingrowth into and onto the porous coralline microstructure or voids left behind during resorption [33]. Callus formation around an implant in the segmental defect treated with a ceramic cylinder that had been loaded with mesenchymal stem cells was reported [3]; similar observations were not made in the present study. It is conceivable that TCP/PLGC membrane might interrupt vascular ingrowth around implant and callus formation.
Histomorphological examinations conducted 12 weeks after the implantation of mixture of β-TCP and cells revealed significantly greater area of new bone formation than control (p < 0.05) and a smaller amount of residual TCP. Previous studies showed that bone marrow-derived MSCs are capable of forming bone in vitro [12,13], and when implanted in an appropriate matrix ectopically or orthotopically [3,14]. Implants with autologous bone marrow MSCs contain more new bones within and around implants in canine segmental bone defect [3]. While undifferentiated adipose derived stromal cells with β-TCP does not affect bone regeneration [20], canine UCB-MSCs presently produced a contrary result.
In a study involving athymic rats, human UCB-MSCs displayed osteogenic differentiation in vitro, survived after xenotransplantation and differentiated into osteoblasts that filled the bony defects [10]. A recent study reported that human UCB-MSCs have a significantly stronger osteogenic potential but less capacity in adipogenic differentiation than bone marrow MSCs in vitro [4]. Presently, canine UCB-MSCs might have enhanced new bone formation by differentiating to osteoblast progenitors. Alternatively, a paracrine effect of canine UCB-MSCs may have enhanced new bone formation. Analyses of bone marrow MSCs with real-time polymerase chain reaction and of bone marrow MSC-conditioned medium by antibody-based protein array and enzyme-linked immunosorbant assay indicated that bone marrow MSCs secrete distinctively different cytokines and chemokines such as vascular endothelial growth factor (VEGF), insulin-like growth factor-1, epidermal growth factor, keratinocyte growth factor, angiopoietin-1, stromal derived factor-1, macrophage inflammatory protein-1alpha, -1beta and erythropoietin, compared to dermal fibroblasts [5]. Several cytokines, chemokines and growth factors are produced during in vitro osteogenic differentiation from human UCB-MSCs, with VEGF being perhaps the most critical driver of vascular formation during osteogenesis [26]. VEGF also stimulates osteoblast proliferation, migration and differentiation [23]. These cytokine alterations accelerate osteogenesis [16,19,30,35]. Further studies will be needed to elucidate the mechanism of bone formation by canine UCB-MSCs.
In a cortical allograft, the host-graft interface heals within 3 months [11]. Vascular invasion begins at the interface and progresses toward the center of the graft. Remodeling of the graft takes months to years, depending on the length, and might never be complete [24]. In the present clinical case, bone lysis and instability of the fractured site was evident by 9 weeks after cortical allograft. After injection of canine UCB-MSCs, bone regeneration gradually appeared in defect sites. Although there was some doubt whether bone formation was attributable to the introduced canine UCB-MSCs or to an endochondral sequence, the injected canine UCB-MSCs injected might play a role in osteoconduction in the graft site.
The results of the present study demonstrate that canine UCB-MSCs accelerate new bone formation upon the implantation of β-TCP into segmental defects in dogs. Implantation of allogenic UCB-MSCs with β-TCP holds promise in the clinical repair of segmental bone defects and non-union fractures.




 XML Download
XML Download