

 PDF
PDF ePub
ePub Citation
Citation Print
Print


During embryonic development, the mesonephric (Wolffian) ducts may persist close to the myometrium of the uterus and muscular wall of the vagina. Imperfect regression of the Wolffian ducts can result in urogenital abnormalities [5,7,8]. Gartner duct cysts develop from the distal remnant of the Wolffian ducts of the vagina. The presence of a persistent Gartner duct cyst of the vagina is rare in dogs. Siddorn and Mann [9] described dysuria in a four-year old springer spaniel with a cyst in the vagina confirmed to be of urogenital origin and Cauvin et al. [1] reported vaginal cysts causing tenesmus in a bitch. Gartner duct cysts are relatively uncommon causes of dysuria in the bitch, and a persistent Gartner duct cyst is extremely rare [3]. This report describes the clinical and pathological findings in a bitch with dysuria and dyschezia due to a large Gartner duct cyst.
A 5 year-old Yorkshire terrier bitch was referred to the Haemaru Referral Animal Hospital with dysuria and dyschezia. On physical examination, the bitch was depressed and a palpable smooth non-painful mass was noted in the caudal region of the abdomen. The radiographic examination showed a round shaped soft tissue mass caudal to the urinary bladder (Fig. 1).
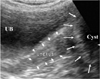
The ultrasound showed a large anechoic fluid filled cyst that was distinct from the uterus. The perineal scan showed that the cyst extended caudal to the vagina (Fig. 2). Results of the CBC, serum chemistry and urinalysis were within reference ranges. The cyst was not suspected as being connected with the vaginal lumen or urethra because there was no clinical sign of vaginal discharge or urinary incontinence. However, surgical resection of the cyst was recommended to eliminate the dysuria and dyschezia. During surgery the cyst was found to be attached to the outer wall of the caudal vagina and there was no opening to the vaginal lumen. About 30 ml of light yellow cystic fluid was removed first and the cystic wall was then resected. Next, the remnant cystic wall was omentalized to prevent a recurrence (Fig. 3). Analysis of the cystic fluid showed that it was a transudate (total nucleated cell count < 500/µl, specific gravity = 1.017, and total protein = 1.6 g/dl). Antibiotics and analgesics were continued for 5 days after the surgery.
The cyst consisted of non-ciliated low columnar epithelial cells consistent with a Wolffian duct remnant (Fig. 4). There were no neoplastic changes or inflammation. After the surgical resection, the clinical problems resolved and no recurrence occurred over 7 months of follow up.
Gartner duct cysts have not been recognized as an important cause of dysuria and dyschezia in dogs because they are extremely rare; [1,4] when present the cysts are usually asymptomatic [2]. While the most common type of vaginal cyst is an inclusion cyst, lined by stratified squamous epithelium, Gartner duct cysts have mucus producing columnar epithelial lining. Therefore, the identification of a Gartner duct cyst is important clinically because dysuria, dyschezia, tenesmus, pain, and dyspareunia can occur with an increase in the size of the cyst [1]. Although aggressive procedures are not recommended usually for asymptomatic cases, this dog had an unusually large Gartner duct cyst that caused mechanical interference with urination and defecation. Treatment was needed to drain the cyst fluid and remove the cystic wall.
Masses in the vagina should be evaluated to differentiate a tumor from a Gartner duct cyst. Smooth muscle tumors are more frequently found in the caudal region of the vagina or vestibule with the masses protruding through the vulva. They are easily noted on clinical examination [6]. Most Gartner duct cysts are benign. However, a biopsy may be necessary to rule out a vaginal malignant tumor, especially if the mass appears to be solid. A vaginal cyst may be mistakenly diagnosed as pyometra, a uterine tumor or a double bladder because of the anatomical location adjacent to the uterus and bladder. An accurate diagnosis can be obtained by radiography and ultrasonography in order to provide proper treatment.
In asymptomatic cases with a Gartner duct cyst, aggressive procedures are not usually recommended. However, the case reported in this study shows that a large Gartner duct cyst in the vagina can cause dysuria and dyschezia in a dog. Symptomatic large Gartner duct cysts require an accurate diagnosis and surgical resection to treat the clinical symptoms.



 XML Download
XML Download