

 PDF
PDF ePub
ePub Citation
Citation Print
Print


In the fetus, the ductus arteriosus develops to divert blood from the not yet functioning fetal lungs back into the systemic circulation. After birth, the ductus arteriosus is closed by a rapid increase in arterial oxygen tension, once the animal starts to breathe. Patent ductus arteriosus (PDA) is the first or second most common congenital heart defect in dogs; it is characterized by failure of spontaneous closure of the ductus arteriosus [7,8].
Surgical ligation of the ductus arteriosus was the most common method used to correct this congenital defect before the introduction of transarterial coil embolization in veterinary practice. Since this procedure does not require open thoracic surgery, it has dramatically reduced the mortality caused by hemorrhage or sudden cardiac arrest. Transarterial PDA coil embolization is a safe, cost effective, less invasive alternative treatment offered by many specialty centers for PDA occlusion. This procedure involves catheterization of the femoral artery under general anaesthesia. An angiogram is then performed to delineate PDA morphology and facilitate coil selection. Coils are commercially available and composed of surgical stainless steel with prothrombotic poly-Dacron fibers. Coils are advanced through a catheter into the PDA under fluoroscopic guidance until satisfactory angiographic occlusion is documented.
The common problems encountered with this procedure are inadvertent pulmonary arterial or aortic embolization, incomplete occlusion and technical difficulties with vascular access in very small dogs. Since deployment of occlusion coils is achieved by catheter manipulation and extrusion of the coil with a guide wire, the accidental release of detachable coils often results in inadvertent pulmonary arterial or aortic embolization [5]. Although pulmonary embolization may not cause life-threatening complications, aortic embolization can cause severe complications including sudden paralysis of the hindquarters.
In this case report we describe a method of retrieval of a coil accidentally dislodged that migrated to the abdominal aorta where the renal arteries branch using a foreign body forceps with a three-wire nail tip.
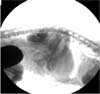
Case history and clinical findings: A 3.5-year-old neutered female miniature poodle (body weight 2.7 kg) was referred to the Veterinary Teaching Hospital at Kangwon National University, because of inadvertent aortic embolization by occlusion coils used in the closure of a patent ductus arteriosus (PDA). On physical examination, the dog showed no apparent clinical signs caused by either heart failure or thromboembolism, except for a V/VI left basal continuous murmur. No apparent abnormalities were observed on the pre-anesthetic laboratory tests. Fluoroscopic examination showed that the coil was lodged at the abdominal aorta where the renal arteries branch (Fig. 1). Because aortic embolization can cause total occlusion of the blood supply to the hindquarters, we decided to remove the coil.
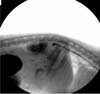
Retrieval of the coil: The dog was premedicated with atropine 0.05 mg/kg SC and acepromazine 0.5 mg/kg IV followed by induction of anesthesia with thiopental 10 mg/kg IV. After tracheal intubation, the anesthesia was maintained with isofluorane at a 2% concentration. To expose the carotid artery, a left lateral incision was made from the third to the sixth cervical vertebrae. After exposing the carotid artery, two spay sutures were made between the cranial and caudal ends of the exposed carotid. A small longitudinal incision was then made to insert a guide wire. After placing the guide wire, the sheath (Check-Flo performer introducer sets; Cook Critical Care, USA) was inserted through the guide wire. After placing the sheath, a foreign body forceps with a three-wire nail tip (Rosot, USA; Fig. 3A) was inserted through the sheath placed at the carotid artery using fluoroscopic guidance (Fig. 2). The occlusion coil was successfully removed (Fig. 3). After removal of the coil, the dog was medicated with heparin at 150 U/kg IV q 8 h and cefazoline at 20 mg/kg IV q 8 h for 3 days, and then released with a prescription for aspirin at 10 mg/kg PO q12 h and cefaclor 10 mg PO q 8 h for 1 week. No apparent clinical signs related to aortic embolization were observed after 10 days from the initial visit.
The occlusion of a PDA, using an embolization coil, is a simple and effective alternative to thoracotomy in young dogs with a small PDA. To date the success rate of this technique has been promising. The major complication rate has been acceptably low, consisting mainly of residual shunting, poor coil positioning and accidental pulmonary or aortic embolization in dogs [2,3,6,9-11]. In humans, the cardiovocal syndrome, which is caused by impingement on the left recurrent laryngeal nerve, by inappropriately placed coils, is a well-known complication after transcatheter coil closure of a PDA; however, this has never been reported in veterinary literature [4]. Any coil that does not appear to be in a stable and satisfactory position should be removed without hesitation; although coils that accidentally are embolized in the lungs can be ignored or pushed to a peripheral location [7]. Therefore, it is essential that appropriate retrieval tools are available. In human medicine, the Amplatz Gooseneck Snare (Microvena, White Bear Lake, USA), Curry snares and small vascular baskets have been used to retrieve dislodged coils [1]. However, a method for retrieval of dislodged coils has never been reported in veterinary literature. In this case report, we successfully retrieved a dislodged occlusion coil from the abdominal aorta under endoscopic guidance, using foreign body forceps, originally designed to retrieve foreign bodies in the airway or gastrointestinal tract. Compared to the retrieval devices used in human medicine, it is cheaper, semi-permanent and relatively easily manipulated.

 XML Download
XML Download