

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Peritonitis is inflammation of the peritoneum. It is different from the inflammatory changes brought about by this condition, and is followed by acute changes in the function of the peritoneum. Peritonitis still continues to be one of the major abdominal emergencies causing high inhospital morbidity and mortality rates of up to 38%. The mechanism for peritonitis is not well established, but its clinical consequences can be quite devastating [4,5,12]. The intraperitoneal administration of live bacteria such as E. coli results in septic peritonitis, with diaphragmatic lymphatic clearance, and systemic bacteremia and endotoxemia [7,8]. In addition, it has been reported that chronic peritoneal inflammation can be induced by an intraperitoneal inoculation of chemical stimuli such as cyanate [11]. However, although these reports have provided valuable information, an animal model with little clinical importance was used in those studies because direct intraperitoneal approaches using these pathogens rarely occur. Although experimental peritonitis was induced by an intraperitoneal injection of several substances, including bacteria [14,18] and chemical stimuli [6,19], the precise mechanism leading to peritonitis is unknown. The lack of a suitable in vivo model for peritonitis has hampered studies aimed at clarifying the mechanism and establishing treatments for peritonitis. Therefore, a convenient and reproducible murine animal model is needed for experimental peritonitis. The overall aim of this study was develop an experimental model for peritoneal inflammation in a murine species using an oral dose of indomethacin.
Materials and Methods
Animals
Specific pathogen-free (SPF) 5-week-old male and female ICR mice and SPF 5-week-old male and female Sprague-Dawley (SD) rats were purchased from Samtako (Osan, Korea). In addition, SPF 5-week-old male and female Mongolian gerbils (Meriones unguiculatus) were obtained from the SPF Animal Facilities, College of Medicine, Seoul National University, Korea. All the animals were allowed to acclimatize in the inspection facility for 1 week before the experiments. Thereafter, the animals were kept in an isolated SPF barrier room with a regulated temperature (23 ± 1℃), humidity (50 ± 5%) and light/dark cycle (12/12 h). The animals were fed a pellet diet sterilized with 2 M rad radiation (Purina, Korea) and sterilized water ad libitum. All the studies were performed in accordance with the Guide for Animal Experimentation, Seoul National University and were approved by the Institutional Animal Care and Use Committee of Seoul National University. All efforts were made to minimize the level of pain or discomfort of the animals.
Experimental design
Twenty-four Mongolian gerbils were divided into four groups. Each group consisted of both males (n = 3) and females (n = 3). The gerbils in group 1 received an oral dose of 1% carboxy methyl cellulose (CMC; Aldrich, USA). The gerbils in the other groups were dosed orally with different concentrations of indomethacin (Fluka GmbH, Switzerland). The concentrations were 20 mg (group 2), 30 mg (group 3) and 40 mg (group 4) per animal body weight in kg suspended in 1% CMC. In the case of the ICR mice and SD rats, the animals were divided into four groups per species and treated with indomethacin in the same manner as described above for the gerbil experiment.
Monitoring of clinical signs, urine analysis and blood sampling
The clinical signs of the animals were assessed twice daily after administering the indomethacin. The animals were sacrificed 5 days after the initial dose. Prior to sacrifice, urination was stimulated by palpation of the lower abdomen, and urinalysis was performed using reagent strips (Multistix 10 SG; Bayer, USA) according to the manufacturer's instruction. The animals were then anesthetized by the inhalation of diethyl ether (Samchun, Korea). The abdomen was then opened, and blood was withdrawn from the lower caval vein using a sterile syringe, transferred to tubes containing 15% EDTA (K3) and immediately cooled on ice. The blood was used for hematology and chemical analyses. Plasma for these analyses was collected by centrifugation at 3,000 × g for 10min at 4℃, and aliquots were stored at -20℃.
Macroscopic and histopathological analysis
Shortly after blood sampling, the animals were sacrificed by a cervical dislocation. After a careful macroscopic inspection, samples from peritoneum and other parenchymatous organs were removed, fixed in 10% buffered neutral formalin, and embedded in paraffin for routine histopathological processing. Four-micron thick sections were stained with hematoxylin and eosin. Two independent investigators, who were blinded to the groups, performed the histopathological examination on coded samples. The level of inflammation and damage was scored by screening each entire peritoneum or the following parameters: fibrosis, inflammatory cell infiltration, and edema. Each parameter was graded on a scale from 0 to 3 as follows: 0, absent; 1, mild; 2, moderate; and 3, severe. The total histopathology score is expressed as a sum of the scores for all parameters. In addition, a histopathology observation was performed on the other parenchymatous organs including the liver, stomach, duodenum, jejunum, ileum, colon, lung, heart, spleen, urinary bladder, kidney, thymus, adrenal gland, cerebellum and cerebrum.
Hematological and biochemical analysis
Hematological analysis was performed using an automatic counter (ADVIA 120; Bayer, USA) according to the manufacturer's instructions. Serum biochemical analysis of the gerbils was performed using an automatic analyzer (DRI-CHEM FDC3500; Fuji, Japan) according to the manufacturer's protocol.
Results
Mongolian gerbils
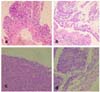
The Mongolian gerbils in the groups given high indomethacin doses (30 mg/kg group 3 and 40 mg/kg group 4) showed swelling of the abdomen, depression and dyspnea within 4 days after treatment. In group 4, two gerbils died on day 5. The severity of the clinical symptoms increased with time. The Mongolian gerbils showing clinical symptoms were necropsied on the 5th day after the initial oral dose. The sacrificed animals were subjected to macroscopic and histology analyses. The animals were confirmed as having developed peritonitis based on the pathological features of the abdominal cavity. The severity of peritonitis increased with increasing indomethacin dose and was not related to gender. The macroscopic findings consisted of abdominal swelling, ascites, swelling of the colon and fibrinous adhesion of the abdominal organs (Fig 1a). The parietal peritoneum was thickened and the digestive tracts were covered with a thin fibrinous film. The liver had a dark color with whitish patches and a dull edge. The gastrointestinal loops adhered to each other along the entire length (Fig 1b). The mesentery was contracted and thickened. Figures 2a and 2b show the histopathological findings in the peritoneum of the gerbils belonging to groups 3 and 4 five days after the oral administration of indomethacin, respectively. The parietal peritoneum was thickened and edema was observed under the mesothelium. Fibrosis also progressed under the mesothelium with the infiltration of mononuclear cells (Fig 2a & b). The histopathological scores shown in Table 1 were higher in group 3 and 4 than in group 2. Inflammatory lesions were observed mainly on their serous surfaces of the other abdominal organs. The livers from groups 3 and 4 showed a thickened serous membrane mainly due to collagen deposition and fibrosis (Fig 2c). There was fibrosis of the visceral peritoneum and infiltration of mononuclear cells in the pancreas of these animals (Fig 2d). Similarly, the animals of groups 3 and 4 showed dark red and sticky material in the jejunum, ileum and enlarged colon. Histopathologically, the jejunum of these animals contained mucosal erosions and hemorrhagic lesions. The animals belonging to the groups given the high dose showed regenerative gastric ulcers in the stomach. However, there were no significant lesions in the other parenchymal organs including the kidney, heart and lung. The animals in group 2 showed mild histopathological changes in the peritoneum (Table 1).
The animals in groups 3 and 4 showed hematological changes such as a significant increase (p < 0.05) in the white blood cell count and a significant decrease (p < 0.05) in the platelet count (Table 2). Biochemical analysis showed a decrease in the total protein and albumin level with a significant increase (p < 0.05) in the alanine transaminase (ALT), asparate transaminase (AST), and blood urea nitrogen (BUN) and creatinine levels (Table 3). Urinalysis revealed mild protein loss.
SD rats and ICR mice
There was no peritoneal inflammation in the SD rats in this study even in those animals given a high dose (Table 1). There was also an absence of peritoneal inflammation in the mice (Table 1). Although sudden death occurred in the group of mice given a high dose of the drug, the pathological lesions were not related to peritonitis. These mice showed severe hemorrhagic changes in the gastrointestinal tract.
Discussion
Despite the advances in diagnosis, surgery, antimicrobial therapy, and intensive care support, the mortality rate in humans with severe peritonitis remains high [4]. In this study, the macroscopic findings of induced experimental peritonitis in Mongolian gerbils were similar to those of clinical peritonitis observed in humans. The parietal peritoneum was thickened and adhered to the abdominal organs. The entire gastrointestinal tract was covered with a thin fibrous film and the mesentery was thickened and contracted. The use of the Mongolian gerbil as an animal model for peritonitis might contribute to determining the mechanisms of clinical peritonitis in humans, and may also help in establishing the therapeutic treatment by screening drugs for preventing peritonitis.
In this study, an animal model, the Mongolian gerbil, was used to develop experimental peritonitis using an oral dose of indomethacin, a nonsteroidal anti-inflammatory drug (NSAID), which is widely used as an analgesic, anti-inflammatory and antipyretic. The main concern for these drugs is the frequency and severity of their digestive side effects involving the entire gastrointestinal tract. The fecal calprotectin is altered in 44% [17] of patients taking NSAID, and scintigrams suggest the presence of small intestinal inflammation in 42% of cases. However, when fecal excretion of [111In]-labeled leukocytes was used as a measure of inflammation, up to 67% [13] of patients were found to have enteropathy. Similarly, in a post-mortem study, intestinal lesions were detected by enteroscopy [10] in 66% of patients, and 13.5% of subjects had nonspecific intestinal ulceration [1]. The intestinal lesions caused by NSAID can mimic inflammatory bowel disease [9] and might lead to chronic bleeding, protein loss, strictures, diverticulitis, appendicitis, internal fistulas, and a relapse of inflammatory bowel disease. The pathogenesis of NSAID enteropathy is complex and is not completely understood. There are two main pathogenic mechanisms. The first involves specific biochemical damage to the mitochondria [15] with uncoupling of the oxidative phosphorylation reaction. This increases the intestinal permeability and the release of calcium into the cytosol, which in turn causes secondary biochemical damage [2]. The second, and more controversial mechanism involves the inhibition of cyclooxygenase (COX)-1 and/or COX-2 and its products (prostaglandins). However, some studies have reported that COX inhibition is not involved [3], while another study suggested that COX inhibition is the key event [16]. In this study, indomethacin induced the dose-dependent and time-dependent formation of macroscopically apparent peritoneal lesions in Mongolian gerbils. Grossly, these animals showed dark red and sticky material in the jejunum, ileum and an enlarged colon. Histopathologically, the jejunum of these animals had mucosal erosions and hemorrhagic lesions. Histopathological scores of peritoneal inflammation were significantly increased by the administration of indomethacin (p < 0.05). Also, peritonitis was revealed by the significant changes of WBC and platelet count (p < 0.05). The results of biochemical analysis were evidenced the hepatic and renal damages in group 3 and 4. The cause of the peritonitis in this study suggests that it might be due to the increased permeability of the jejunum caused by the administration of indomethacin. Both total protein albumin level and histological findings could suggest it.
This study found an effective and simple method of inducing peritonitis by oral dosing of indomethacin at a rate of 30 mg/kg body weight using 5-week old Mongolian gerbils. The resulting peritonitis that developed can be used as an effective tool for investigating the potential therapeutic compounds aimed at preventing peritoneal damage during peritonitis and provide insight into the pathophysiology of peritonitis.




 XML Download
XML Download