

 PDF
PDF Citation
Citation Print
Print


Introduction
Tracheal collapse (TC) is a congenital cartilaginous tracheal ring problem to which small-breed dogs are predisposed. It is usually diagnosed by performing radiography, fluoroscopy, and tracheobronchoscopy. Tracheobronchomalacia is a structural defect of the trachea and bronchial cartilages. It results in flattening of the trachea and bronchial lumen. Affected tracheae show hypocellularity of the cartilages, loss of hyaline cartilage, and deficiencies of chondroitin sulfate, calcium, and glycosaminoglycans [7]. Fifty-one percent of dogs with a chronic cough exhibit tracheobronchomalacia, a condition regarded as a common cause of cough. More toy-breed dogs than dogs of other breeds show tracheobronchomalacia when they have a chronic cough [13]. Upper airway obstruction, infectious tracheobronchitis, heart enlargement, parasitic disease, obesity, and oral problems can exacerbate clinical signs of TC [12]. However, studies investigating TC in patients without a history of cough are lacking.
Lung hernia is a protrusion of the lung parenchyma beyond the boundaries of the thoracic cavity [18]. Lung hernia can be classified by its etiology and location in humans [19]. It may appear as congenital or acquired (spontaneous or traumatic), and it can be classified as cervical, thoracic, or diaphragmatic hernia based on its location. In human medicine, cervical lung hernia usually occurs during infancy or childhood and disappears spontaneously as time passes. It may be unilateral or bilateral, and, particularly, right lung hernias occur three times more frequently than left lung hernias [22]. Partial absence, laxity, or attenuation of Sibson's fascia results in acquired cervical lung herniation (CLH) with protrusion of the lung between the anterior scalene and sternocleidomastoid muscles [1618]. There are no reports describing the anatomy of canine CLH. Most cases of acquired cervical lung hernias in humans occur due to penetrating chest trauma or surgery, chest wall neoplasms, or chest wall infections. However, studies have shown that 29% of acquired cervical lung hernias can appear without any particular event and can occur due to chronic cough or repeated Valsalva maneuvers [1718]. CLH is a common phenomenon in dogs, but sufficient reports regarding the factors influencing CLH are lacking [4561120]. In contrast to human studies, previous reports in dogs have shown that there was no significant relationship between the duration of cough and CLH, although there was a strong association between intrathoracic TC and CLH [20].
The purpose of the present study was to investigate the fluoroscopic characteristics of TC and CLH in dogs and to determine the presence of potential relationships with various influencing factors.
Materials and Methods
Case selection
Cases with fluoroscopic and radiographic images of the trachea that presented to the Veterinary Medical Teaching Hospital of Seoul National University between 1 January 2012 and 31 December 2015 were retrospectively evaluated, and the medical records for each case were reviewed. Cases with an obvious history of cough and a normal chest conformation, as determined by lateral radiographs, fluoroscopic images in lateral and ventrodorsal recumbency, and an inducible coughing phase during fluoroscopic examination, were included. In the absence of a coughing phase in fluoroscopy, TC may be underestimated, and such cases were excluded. If fluoroscopic examination was performed several times in one patient, each exam was considered as an individual case.
Medical records review
For each dog, signalment, cough history, presence or absence of a heart murmur, and chief complaint were recorded. In order to evaluate the association between CLH and duration of cough, chronic cough cases were defined as those with a cough lasting longer than 2 months [13].
Fluoroscopic image evaluation
Images of the patients' normal respiration status and forceful expiration (coughing) status were obtained through fluoroscopic examination. With the dogs carefully positioned in right lateral recumbency, the normal respiratory phase was evaluated, and the cervical trachea was subsequently compressed for evaluation of the coughing phase. In order to investigate CLH, images were acquired during the coughing phase with the patients in humanoid position.
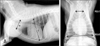
The location and grade of TC, grade of CLH, and kinking of the trachea were evaluated by an author (J Lee). If the tracheae lost their linear shape and showed a curved appearance, they were included in the tracheal-kinking group. The trachea was divided into cervical, thoracic inlet, intrathoracic, and carinal regions. In this study, the mainstem bronchi were also included in the evaluation of TC, and TC was graded as 0%–25% (Grade 1), 25%–50% (Grade 2), 50%–75% (Grade 3), and greater than 75% (Grade 4) by determining the decrease in luminal diameter. The mainstem bronchi were assessed only for the presence or absence of collapse. CLH was graded as Grade 1 (7th cervical vertebra), Grade 2 (6th cervical vertebra), Grade 3 (5th cervical vertebra), and Grade 4 (4th cervical vertebra, Fig. 1) by comparing the herniated apical level of the cranial lung lobe to the cervical vertebral body in humanoid view. If the lungs protruded into the level of the intervertebral disc space, the cranial vertebral body was used to decide the grade of CLH.
Radiographic image evaluation
At least two thoracic radiographs in ventrodorsal and right lateral recumbency were obtained for each case. To investigate the relationship between chest conformation and CLH, several diameters were measured on digital radiographs. The diameter of the thoracic inlet on lateral view was measured from the ventral margin of the vertebral body at the midpoint of the most cranial rib to the dorsal margin of the manubrium at the level of minimal thickness [14]. Thoracic depth was the distance from the dorsal aspect of the xiphoid process to the ventral aspect of the vertebral body perpendicular to the line from the xiphoid process. Thoracic width was the distance between the medial borders of the 1st and 8th ribs (Fig. 2). Thoracic depth to width ratio at the level of the 8th rib (depth/Rib8), thoracic inlet distance to thoracic depth ratio (LAT ratio), and the ratio of thoracic widths at the level of the 1st and 8th ribs (VD ratio) were calculated [15]. Cases having pectus excavatum and ill-defined sternebrae were difficult to measure; therefore, these cases were excluded.
Statistical analyses
A chi-squared test was used to investigate the association between TC and the patients' history of cough. The Mann-Whitney U test was used to determine differences in age between cases with and without TC. Analysis of CLH and influencing factors (age, chronic cough, a history of cough, tracheal collapse, kinking of trachea) was performed by using Fisher's exact, chi-squared, and Mann-Whitney U tests and logistic regression. Age and chest conformation ratios are presented as mean ± SD values. The independent t-test was used to assess the relationship between presence of CLH and chest conformation and between CLH and breed. A value of p < 0.05 was considered statistically significant. All statistics were calculated by using SPSS (ver. 23; IBM SPSS Statistics; IBM, USA).
Results
Fluoroscopic examination for differentiation of TC was performed in 391 dogs between 1 January 2012 and 31 December 2015. Among these, 222 dogs met the inclusion criteria for this study. Among the study population, fluoroscopic examination was performed twice in ten patients. Sixteen breeds were included (Table 1) and the average age was 10.73 ± 3.17 years (range, 1 to 18 years). Eighty-eight neutered male (39.6%), 74 spayed female (33.3%), 39 intact female (17.6%), and 21 intact male (9.5%) dogs were included in the study. There was no sex predisposition detected.
Tracheal collapse was observed in 199 cases (89.6%), CLH presented in 124 cases (55.9%), cardiac murmur was detected in 76 cases (34.2%, 13 cases had unknown history about cardiac murmur), and tracheal kinking was present in 65 cases (29.3%). There were 147 cases (66.2%) with a history of cough.
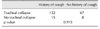
Tracheal collapse was most commonly observed in the carinal region (173 cases, 77.9%), followed by the mainstem bronchus (164 cases, 73.9%), intrathoracic tracheal region (122 cases, 55.0%), thoracic inlet region (90 cases, 40.5%), and cervical region (48 cases, 21.6%). Dogs with TC (10.87 ± 3.12 years) were older than dogs without TC (9.43 ± 3.36 years; p = 0.047). There was no association between having a history of cough and TC (p = 0.915, Table 2). Many cases exhibited TC without a history of cough.
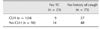
The left lung (113 cases, 50.9%) had more CLH than the right lung (79 cases, 35.6%), and bilateral CLH was noted in 68 cases (30.6 %). Grade 1 CLH (69 cases) was most commonly observed, followed by grade 2 (43 cases), grade 3 (9 cases), and grade 4 (3 cases). Dogs with CLH (11.28 ± 2.62 years) were older than dogs without CLH (10.02 ± 3.64 years; p = 0.004). A greater proportion of Pekingese (3/3, 100%), Shih Tzu (31/38, 81.6%), Miniature Pinscher (3/4, 75.0%), Cocker Spaniel (4/6, 66.7%), Yorkshire Terrier (26/43, 60.5%), and Pomeranian dogs (9/17, 52.9%) had CLH than that in mixed-breed dogs (6/13, 46.2%, Table 1). The breeds with the greater percentage incidence of CLH were defined as predisposed breeds in the present study. Univariable analysis revealed that CLH was associated with having a history of cough (p < 0.001), intrathoracic TC (p = 0.008), kinking of the trachea (p < 0.001), and a greater age (p = 0.010). In contrast, CLH was not associated with TC (p = 0.088) or chronic cough (p = 0.622). Although there was an association between CLH and having a history of cough, it is particularly notable that CLH was observed in 36.0% of dogs without a history of cough (27/75, Table 3). Tracheal kinking (p < 0.001) and having a history of cough (p = 0.001) were associated with the grade of CLH. Patients with higher grades of CLH had a greater incidence of tracheal kinking and a history of cough (Figs. 3 and 4). Results of multivariable analysis indicated that tracheal kinking, cough history, and age were significant risk factors for CLH (Table 4). In addition, LAT ratio (p = 0.001) was higher in the study's predisposed breeds than in other breeds (Table 5).
Discussion
There are currently no reports grouping CLH by severity in dogs. The present study assessed CLH grade to determine the effect of CLH severity. Due to breed variations, relative values based on the vertebral body were used instead of absolute values. In the present study, the majority of examined cases were small-breed dogs, which is consistent with previous studies [4567111320]. However, since the majority of patients referred to this institute are small-breed dogs, the results may have been affected by the composition of the population. In this study, cases with TC and CLH were of greater age than cases without TC and CLH. It should be noted that there was no association between TC and a history of cough. Many patients that coughed during physical examination or showed a narrowed airway on radiographs had TC but no cough history. Therefore, it is important to rule out TC through a combination of physical examination and diagnostic imaging, especially when the patient may undergo anesthesia, because TC can lead to life-threatening situations. In human medicine, anesthesia is regarded as a difficult procedure in patients with tracheomalacia [1]. Although the risks associated with TC and anesthesia have not been reported in dogs, TC can be an important cause of mortality during the postoperative period. In TC patients, the extent of collapse can be worsened by excitation and respiratory distress after extubation, which can result in a vicious cycle of further collapse, excitation, and distress. Therefore, pre-anesthetic information regarding the presence of TC is important when planning a patient-based anesthetic protocol.
In humans, cervical lung hernia is uncommon. It presents in 25% of all lung hernias and is usually a congenital problem that disappears spontaneously [10]. In adults, many cervical lung hernias result from chest trauma or surgery, chest wall neoplasms, or chest wall infections [17]. Twenty-nine percent of acquired cervical lung hernias occur in the absence of any special events and are associated with increases in intrathoracic pressure resulting from chronic cough, emphysema, and repetitive respiratory maneuvers [1718]. CLH was known as a rare phenomenon in dogs, and there are only 126 reported cases of dogs with CLH [4561120]. However, in one previous report, CLH was evaluated in 121 cases by fluoroscopy, and 70% of the cases were diagnosed with CLH. In that study, there was no association between CLH and duration of cough [20]. In the present study, the number of cases that presented without a history of cough was sufficient to allow evaluation of the relationship between cough and CLH. The results showed that CLH was significantly correlated with having a history of cough, intrathoracic TC, tracheal kinking, and age. However, many of the dogs without a history of cough (27/75, 36.0%) had CLH, a result that should not be ignored. Therefore, factors other than cough history may be associated with CLH. Age was a significant risk factor for CLH in this study. As has been reported in humans, increased muscle weakness with aging may be an important factor influencing CLH in dogs [39]. If thoracic muscles are already weakened, even a transient cough could cause the cervical lung lobe to protrude beyond the thoracic cavity. In addition, repeated barking could cause increased pressure within the thoracic cavity. Moreover, breed predisposition may be another risk factor for CLH. In previous case reports, 40% (2/5) of lung herniation cases were in Pekingese dogs [45611], and, in the present study, all Pekingese dogs that met the inclusion criteria had CLH. Differences in thoracic anatomy can be a cause of CLH as well. However, there are currently no reports describing the anatomy of lung herniation in dogs, nor reports comparing the thoracic anatomy of Pekingese dogs to those of other breeds. According to a previous study, CLH had no specific association with breed or chest conformation [20]. In the present study, dogs in the study's predisposed breeds had higher LAT ratios or a wider thoracic inlet compared to the other breeds. Therefore, many factors can be causes of the CLH other than cough history, so even though there may be no clinical signs of cough in a small-breed dog, caution is needed when collecting blood from the external jugular vein [2]. Although no association was detected between chronic cough and CLH, having a history of cough, tracheal kinking, and a greater age were associated with CLH in our multivariable logistic regression analysis. Moreover, intrathoracic TC showed a relationship with CLH in our univariable analysis. Intrathoracic TC usually occurs during forced exhalation, and intrapleural pressure increases during exhalation. When this pressure exceeds the pressure in the airway lumen, dynamic collapse can occur. Airway collapse impedes air flow; consequently, the lung lobes protrude with the increase in intrapleural pressure. Tracheal kinking was also associated with CLH grade. Patients with higher grades of CLH had a greater incidence of tracheal kinking. Tracheal kinking may cause damage to the trachea and may be associated with clinical signs of coughing [17]. However, more studies are needed to determine the relationship between tracheal kinking and deformation of the trachea. Although complications related to cervical lung hernias, such as coughing caused by tracheal irritation, dysphagia, incarceration of the lung, and pain due to the compression of nerves, have been reported in human medicine [221], no such complications have been associated with CLH in the present study. However, since coughing was a common sign in the cases presented in this report, and as patient follow-up was not pursued, it is not clear whether tracheal kinking and CLH had an influence on coughing. In veterinary medicine, a single case of dysphagia due to CLH was reported in a juvenile dog [6].
In dogs, since the left cranial lung lobes are located cranial to the right cranial lung lobes, lung protrusion beyond the thoracic cavity is more common in the left cranial lung lobes [8]. Among the cases presented in this report, there was no history of trauma or disease in the cranial thoracic region. Therefore, the etiology of acquired CLH may be different in dogs than in humans, in which thoracic trauma is the most common cause of acquired CLH [1017]. The relationship between lung herniation and intrathoracic TC detected in this study is similar to that previously reported [20]. Since increased intrathoracic pressure is a cause of CLH, and as intrathoracic TC can result in increased intrathoracic pressure during expiration, intrathoracic TC may result in CLH [14].
The main limitation of this study was its retrospective nature. Also, due to the absence of follow-up examinations, it is unknown whether CLH exacerbates clinical signs. Finally, since the majority of cases in this study were small-breed, geriatric patients, further studies are required to determine whether CLH is also common in younger aged dogs.
In conclusion, in patients without a history of cough, TC can be frequently diagnosed through fluoroscopic examination. This is a notable result, especially when determining an anesthetic protocol, because excitation after extubation can induce respiratory distress which can result in further narrowing of the airways and potentially causing a vicious cycle of further excitation, distress, and airway narrowing in patients with TC. Therefore, whether or not patients have a history of cough, physical examination and diagnostic imaging are required in order to rule out TC, particularly in small-breed dogs.
Based on fluoroscopic examination, CLH is a common finding in older dogs. Although coughing is a factor influencing CLH, CLH can appear in dogs without a history of cough. Kinking of the trachea is more common in dogs with severe CLH, and mechanical irritation of the trachea may worsen clinical signs. Therefore, more caution is needed for patients where CLH is severe enough to be detected by physical examination.






 XML Download
XML Download