

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Several studies have demonstrated that the angle between the patellar ligament and tibial plateau (patellar ligament angle, PLA) is correlated with anterior shear forces in the stifle joint [2,5,8]. A previous report [1] showed that the cranial cruciate ligament (CrCL) withstands up to 86% of the anterior shear force. However, no studies have measured the PLA in dogs with complete rupture of the CrCL.
A cranial drawer test or tibial compression test is used to evaluate craniocaudal instability of the stifle joint [7]. Recently, it was determined that the drawer test alone or combined with the tibial compression test could not be used to differentiate the cause of stifle instability associated with CrCL, caudal cruciate ligament, and total cruciated ligament rupture [4]. A stress view radiograph of the stifle is helpful for observing cranial displacement of the tibia in dogs with a ruptured CrCL [6]. However, radiographs are associated with numerous disadvantages such as variation depending on the examiner and difficulty detecting subtle instability. Thus, more objective tools are needed to accurately detect stifle joint disorders. The purposes of the present study were to evaluate and compare the PLA in dogs with intact stifle joints, with CrCL rupture, and a ruptured CrCL repaired by surgery. We developed a quantitative method to evaluate stifle joint instability to help diagnose CrCL rupture.
Materials and Methods
Case selection
The medical records and radiographs of dogs admitted to the Veterinary Medical Teaching Hospital of Konkuk University for CrCL rupture from March 2007 to June 2013 were evaluated retrospectively. Thirty-three stifle joints from 26 dogs showing clinical recovery after extracapsular surgery (ES) were included in this study. Initial inclusion criteria were complete CrCL rupture confirmed during surgery and that the affected stifle joint was stabilized by ES. Dogs with medial patellar luxation (MPL) were included because the affected animals were mostly small breeds. Dogs that had undergone tibial tuberosity transposition as well as ones with meniscal damage, collateral ligament damage, or a caudal cruciate ligament rupture were excluded from the investigation.
Radiographs were evaluated to select dogs with preoperative plain and stress views along with postoperative plain views of the stifle joint within 1 month after surgery. The postoperative stress view was not examined because it was not taken into account during surgery. Radiographs of stifle joints with ≤ 2 mm superimposition of the femoral condyles and little to no degenerative joint disease were assessed.
Control selection
Medical records of dogs presented to the Veterinary Medical Teaching Hospital of Konkuk University from March 2007 to June 2013 were evaluated retrospectively. A total of 105 normal stifle joints from 79 dogs were examined. The animals were confirmed to be free of stifle joint disorders based on medical history, orthopedic examination, and radiographs. Radiographs were evaluated to select dogs with mediolateral views of stifle joints that had a ≤2 mm superimposition of femoral condyles.
Radiographic evaluation
Mediolateral radiographs of stifle joints were digitized for analysis using S View software (ver. 1.5.5.3; Comed Medical Systems, Korea). Preoperative plain and stress mediolateral views of the affected stifle joint along with postoperative plain mediolateral views were obtained. All radiographic views focused on the tibiofemoral joint space and extended at least to the level of the mid-diaphysis of the tibia and femur. Landmarks for measurements were based on those described in a previous study by Dennler et al. [2].
The flexion angle of the stifle joint (β) was measured from two long axes of the femur and tibia that were defined as the lines between the two shafts, midpoints at one-third and two-thirds of the femoral and tibial lengths (Fig. 1). The angle between the proximal border of the patellar ligament and tibial plateau (α) was measured on each radiograph. The tibial plateau line extended from the point on the cranial margin of the tibial plateau at which the CrCL inserted to the point on the caudal margin of the tibia at which the caudal cruciate ligament was inserted. Angles α and β in all patients were evaluated by the same observer. In our preliminary study (unpublished data) evaluating the reliability of measuring the patellar ligament angle, 12 normal stifle joints of six beagles were included. Mediolateral radiographic plain and stress views of the stifle joints were obtained, and plain radiography was performed three times for three groups of flexion angles (angle β 40~60°, 60~80°, and 80~100°). The PLA was evaluated according to stifle joint flexion by three independent observers. Each observer measured three times and calculated the average angle α. Significant differences in the PLA were observed among the flexion angle groups (p < 0.05). No significant difference in PLA was observed between the plain and stress views. The inter-class correlation coefficient of the PLA obtained from each observer was 0.971 (p < 0.05). The intra-class correlation of measurement for the PLA was 0.940 (p < 0.05).
Surgical technique
All dogs underwent lateral or medial parapatellar arthrotomy to explore the affected stifle joint. Remnants of the torn CrCL were resected, and joint lavage was performed with sterile saline. Stabilization procedures using extracapsular methods included lateral fabellotibial suturing along with modified medial and lateral retinacular imbrication techniques. Fisher, polyester, or polyethylene line was used as the implant material. Sutures were manually tied or connected with a crimp. Closure was performed using a routine technique. All patients had resistance to the cranial drawer test and showed complete clinical recovery after surgery.
Statistical analysis
The data analysis was performed using SPSS for Windows (ver. 19.0; SPSS, USA). The mean and range for angles α and β were calculated. Relationships between angles α and β were analyzed by simple linear regression with a 95% confidence interval (CI). PLA preoperative and postoperative views were compared using an independent t-test. The capacity of PLA measurements to identify a CrCL rupture was evaluated using receiver operating characteristic (ROC) curves. Differences were considered significant if p < 0.05.
Results
CrCL rupture group
For the 33 stifle joints, 20 surgeries were performed on the right stifle joint and 13 were conducted for the left stifle joint. Seven dogs underwent bilateral surgery. Twelve stifle joints with CrCL rupture also had MPL and were corrected by trochleoplasty and lateral imbrication with ES. The 26 dogs included four sexually intact females, six neutered females, one sexually intact male, and 15 neutered males. Breeds included Yorkshire terrier (n = 7), Maltese (n = 6), poodle (n = 3), and one each of Shih Tzu, Cocker spaniel, Siberian husky, mixed, Bichon Frise, Coton de Tulear, beagle, chowchow, American Eskimo, and Cane Corso. The mean age of the dogs at the time of surgery was 7.66 ± 2.54 years (range, 3.0~12.0 years), and mean body weight was 9.87 ± 12.49 kg (range, 1.7~52.0 kg).
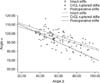
Preoperative angle α of the 33 stifle joints ranged from 68.10° to 109.77° (mean, 89.00 ± 11.00°) and flexion angle β ranged from 39.01° to 98.76° (mean, 62.61 ± 18.26°). Postoperative angle α ranged from 79.41° to 116.71° (mean, 95.86 ± 8.26°) while flexion angle β ranged from 35.01° to 97.78° (mean, 55.48 ± 15.19°). The linear regression equation (Fig. 2) for α versus β before surgery was: α = -0.78β + 118 (r2 = 0.602; p < 0.001). The linear regression equation for α versus β after surgery was: α = -0.56β + 113 (r2 = 0.314; p < 0.001).
Normal group
Mean age of the normal dogs was 6.78 ± 4.10 years (range, 0.5~15.0 years). Mean body weight was 9.37 ± 10.44 kg (range, 1.1~49.0 kg). The breeds included Maltese (n = 25), Yorkshire terrier (n = 10), poodle (n = 7), miniature Schnauzer (n = 1), miniature pinscher (n = 3), Pomeranian (n = 4), beagle (n = 2), white terrier (n = 4), Dalmatian (n = 2), Jindo (n = 3), Siberian husky (n = 1), Pekinese (n = 2), French bulldog (n = 3), Cocker spaniel (n = 8), golden retriever (n = 1), Labrador retriever (n = 5), Chihuahua (n = 3), border collie (n = 1), silky terrier (n = 1), Shih Tzu (n = 4), Bichon Frise (n = 1), American Eskimo (n = 1), and mixed breed (n = 11). The mean angle α was 97.35 ± 7.72°° (range, 75.32~119.44°) and the mean angle β was 58.60 ± 15.45° (range, 27.21~94.04°) for all dogs. The linear regression equation for angles α versus β (Fig. 2) was: α = -0.32β + 116 (r2 = 0.416; p < 0.001).
Comparison of the PLA among dogs with normal, ruptured CrCL, and repaired stifles
Comparisons of the PLA were performed on radiographs taken with a normal standing angle (40~60° flexion angle) and general positioned angle during the radiographic examination (60~80° flexion angle). Extremely extended or flexed stifles were excluded. Significant differences were observed in the PLA between the preoperative plain view and preoperative stress view (p = 0.003), preoperative stress view and normal stifles (p = 0.000), and preoperative stress view and postoperative plain view (p = 0.001) with a 40~60° flexion angle (panel A in Fig. 3). Significant differences in the PLA were also found between preoperative plain view and normal stifles (p = 0.008), preoperative stress view and normal stifles (p = 0.000), preoperative plain view and postoperative plain view (p = 0.039), and preoperative stress view and postoperative plain view (p = 0.002) with a 60~80° flexion angle (panel B in Fig. 3).
ROC curves
The ROC curve for the stress view (panel A in Fig. 4) with a 40~60° flexion angle indicated that the area under the curve (AUC) was 0.949 (95% CI, 0.897~1.000; p = 0.000). If the cutoff value was 92.40°, the PLA measurement had a sensitivity of 90.0% and specificity of 100%. The ROC curve for the plain view (panel B in Fig. 4) demonstrated the AUC was 0.686 (95% CI, 0.500~0.873; p = 0.040). With a 94.51° of cutoff value, the PLA measurement had a sensitivity of 86.0% and specificity of 61.5%.
The ROC curve for the stress view (panel C in Fig. 4) with a 60~80° flexion angle showed that the AUC was 0.945 (95% CI, 0.881~1.000; p = 0.000). With a 90.55° cutoff value, the PLA measurement had a sensitivity of 83.9% and specificity of 100%. The ROC curve for the plain view (panel D in Fig. 4) indicated that the AUC was 0.785 (95% CI, 0.605~0.965; p = 0.004). With a 90.76° cutoff value, the PLA measurement had a sensitivity of 83.9% and specificity of 75.0%.
Discussion
Stifle joint force consists of compressive force and shear force. These forces may vary considerably depending on joint flexion degree. Anterior shear force in stifle joints is greatest at full extension and decreases with stifle flexion. However, the relationship between anterior shear force and the PLA is not completely understood [2,5].
In the present study, the PLA of stifles with a complete CrCL rupture was significantly lower than that of normal stifles. In particular, a significant difference in the PLA between the normal stifle and CrCL rupture groups was observed at a 60~80° flexion angle on both the plain and stress views. For the 40~60° flexion angle group, a significant difference was observed in the PLA between the normal stifle and CrCL rupture groups only on the stress view. Sedation is often required to obtain images of the stress view [7]. Therefore, it would be useful to examine mediolateral plain radiographs of affected stifle joints at a flexion angle of 60~80° to diagnose a CrCL rupture if the dog was uncooperative when imaging the stress view.
Both the preoperative and postoperative PLA in dogs that had a completely ruptured CrCL decreased linearly with increasing stifle joint flexion. These results are consistent with findings from previous studies [2,8]. The linear regression equation for α versus β before surgery was: α = -0.78β + 118 (r2 = 0.602; p < 0.001). The linear regression equation for α versus β after surgery was: α = -0.56β + 113 (r2 = 0.314; p < 0.001). It was possible to predict the angle between the patellar ligament and tibial plateau depending on the stifle joint angle because the preoperative linear formula was relatively well defined (r2 = 0.602). We showed that the postoperative regression line was close to the regression line in intact stifles.
In a previous study, the tibial plateau angle (TPA) was evaluated preoperatively and postoperatively [3]. TPA values were unchanged after ES in dogs with a CrCL rupture. We showed that the postoperative PLA tended to increase to a normal value following surgery. Significant differences in the PLA were observed between the preoperative stress view and postoperative plain view at the 40~60° flexion angle. With a 60~80° flexion angle, the postoperative PLA was significantly greater in not only the preoperative stress view but also the preoperative plain view. These results would be helpful for evaluating surgical outcomes.
The ROC analysis revealed that the stress view had a better AUC for detecting CrCL rupture than that of the plain view. These results suggest that the stress view might be useful for evaluating a complete CrCL rupture. If the PLA is < 90.55° on the stress view with a 60~80° flexion angle, the dog should be diagnosed with a complete rupture of the CrCL with a sensitivity of 83.9% and specificity of 100%. However, no quantifiable methods have been available to evaluate CrCL rupture in dogs until now. One previous report mentioned that the drawer test alone or combined with a tibial compression test is not suitable for identifying stifle instability with a ruptured CrCL [4]. We determined that measuring the PLA is a quantitative method for evaluating stifle joint instability, and is a valuable technique for diagnosing complete rupture of the CrCL in canines.
In conclusion, measuring the PLA is a valuable method for identifying complete rupture of the CrCL. The PLA of dogs with a ruptured CrCL was significantly lower than that of normal dogs. In particular, significant differences were observed in the PLA between the normal stifle and CrCL rupture groups at a 60~80° flexion angle. Therefore, positioning in a 60~80° flexion angle is recommended when taking radiographs to assess complete CrCL rupture. If the PLA is < 90.55° on the stress view with a 60~80° flexion angle, the dog should be strongly suspected to have complete rupture of the CrCL.



 XML Download
XML Download