

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Sedatives and analgesics have been widely used for diagnostic procedures and minor surgery in standing horses [10]. The sedative agents contain alpha-2 adrenergic receptor agonists (α2 agonists), phenothiazines, and benzodiazepines. The analgesic agents are comprised of opioids, α2 agonists, and non-steroidal anti-inflammatory drugs [10]. A veterinarian may choose a drug based on the temperament and physical status of the patient, procedure to be performed, available facilities, drug cost, and/or personal preference [5,10]. Combinations of these drugs have been shown to provide more desirable sedation and analgesia, and decreased side effects than when the drugs are used individually [3,5,10].
The α2 agonists available for horses include xylazine (X), detomidine, romifidine, and medetomidine; they are used for sedation, analgesia, and muscle relaxation [5]. The clinical and cardiopulmonary effects and other complications associated with these drugs are well-known [5,9,10,12,17,20]. Although their principle actions and side effects (e.g., bradycardia, second degree atrioventricular block, respiratory rate decrease, and ataxia) are similar, there are some differences in the duration, degree of action, and complications related to these drugs [5,12,17,20] e.g., the duration of detomidine and romifidine is longer than that of X, and romifidine produces less lowering of the head and a lower degree of ataxia than the other drugs [5,6,12]. Medetomidine is not widely used in equine practice because it produces more pronounced and prolonged ataxia [1,5,20].
Opioid agents, primarily used for their analgesic properties in small animal practices, are of limited use in equine practice because of the possibility of central nervous system (CNS) excitation [2,10]. However, opioids are often used with α2 agonists, the combination of which increases clinical effects and decreases side effects, compared to the individual use of the drugs [3,5,10]. Opioids used in horses include morphine, butorphanol, and buprenorphine [2,3,10]. Mu-agonist opioids are generally considered as the most effective analgesics. In horses, however, the µ-receptor antagonist and κ-agonist opioid butorphanol is most commonly used [5,10]. These drugs are subject to legal control in most countries.
Tramadol (T), a centrally acting analgesic drug that is a synthetic analog of codeine, is not a controlled drug in Korea [16,18]. For the last two decades, T has been used in humans to treat moderate to severe postoperative pain [18]. More recently, T was introduced into veterinary medicine, and has shown analgesic effects in mice, rats, dogs, and cats [11,15,16]. T is also a potential analgesic agent for horses, although there is a paucity of studies addressing its use in this species.
The objectives of this study were to evaluate the sedative and analgesic effects of T in horses and to compare the clinical effects of the combination of XT with the individual drug effects.
Materials and Methods
Experimental animals
Thoroughbred saddle horses (four mares, one stallion, and one gelding), 3- to 7-years-of-age (4.6 ± 1.8 years), weighing 440 ± 27 kg (399~470 kg) were used for this study. The horses were housed in individual stalls at a riding club near the College of Veterinary Medicine, Seoul National University (Korea) where they were fed hay and concentrates and permitted free access to water. Before the experiment, informed owner consent was obtained.
Procedures
The experiment was performed as a randomized, blind, three-way crossover design with at least a 7-day washout period between treatments. Prior to each treatment, the horses were physically examined and weighed. Food, but not water, was withheld for at least 8 h prior to drug administration. During the experiment, horses were placed in stocks and allowed 20 min to acclimate to their surroundings. The hair over the left jugular vein was clipped, and a 16 gauge over-the-needle catheter was placed in an aseptic manner. The left paralumbar fossa region was aseptically prepared with 70% alcohol, and two 20-gauge, 1.5 inch needles were inserted 7 cm apart for analgesic effect assessment. The electrical stimulator was placed at least 2 m away from the horses. Electrocardiogram pads for apex-base lead, rectal temperature (RT) probe, and indirect arterial pressure (IAP) probe at the base of the tail for oscillometry were positioned for data collection. Treatments consisted of X (Xyzine 300; SF, Korea), 1.0 mg/kg; T (Toranzin 50; Samsung Pharm, Korea), 2.0 mg/kg; or a combination of XT 1.0 and 2.0 mg/kg respectively administered intravenously (IV) via a jugular vein catheter. X was given as a bolus, whereas T was slowly injected over at least 2 min. For the XT treatment, the X bolus was followed by a slow T injection. Heart rate (HR), respiratory rate (RR), RT, IAP, capillary refill time (CRT), sedation, and analgesia (using electrical stimulation and pinprick) were measured prior to drug administration and 5, 10, 15, 20, 25, 30, 40, 50, 60, 75, 90, 105, and 120 min after administration. HR, RT, and IAP were measured using a BSM-2301 patient monitor (Nihon Kohden, Japan). RR was evaluated by counting thoracic wall movements for 1 min. CRT was determined by pressing a finger against the horse's upper gums for 2 sec and monitoring color change. Degree of sedation was quantified using a 4-point criteria system in which (1) denoted deep sedation, defined as markedly decreased movement, lower head carriage with mouth to the carpal joint, marked drowsiness, droopy eyelids and lip, and markedly wide based stance; (2) denoted moderate sedation, defined as moderately decreased movement, lower head carriage with mouth to the elbow joint, drowsiness, slightly droopy eyelids and lip, and moderately wide based stance; (3) denoted mild sedation, defined as slightly decreased movement, lower head carriage with mouth to the shoulder, and decreased sensitivity to surroundings; and (4) denoted no sedation, which was considered to be normal behavior and appearance. Analgesic effect was assessed by two methods: the first was electrical stimulation (5.5 mV, 1 Hz, 1 sec) on the left paralumbar fossa with an electrical stimulator (AM-3000, TEC, Japan); and the second was by pinprick with a 20-gauge, 1.5 inch needle on the right neck, right paralumbar fossa, and right hip, which were pricked one by one. Needle prick was continued to the whole length of needle (1.5 inches), but applied just once in only one place. The degree of analgesia was assessed by observing the changes from baseline in responses (i.e., attention to the stimulated site, tail twitch, movement of the head and legs, escape from stimulus, pawing, and kicking). Analgesia was scored on a 4-point scale as follows: 1 = deep analgesia, defined as markedly different responses from baseline (5 or 6 of the observational signs disappeared); 2 = moderate analgesia, defined as moderately different from baseline value (3 or 4 observational signs disappeared); 3 = mild analgesia, defined as slightly different from baseline value (1 or 2 observational signs disappeared); and 4 = no analgesia, in which no response changes were observed. Sedation and analgesic scores of electrical stimulation were expressed using a 4-point scale, but analgesic score of pinprick was the sum (0 to 12) of the 4-point scale of the three sites (the right neck, right paralumbar fossa, and right hip). Sedation and analgesia were measured by a single investigator who was blinded to treatments throughout the experiment.
Statistical analysis
Data are expressed as the mean ± SD. Statistical analysis of data was performed with SPSS 17.0 software (SPSS, USA). The results of HR, RR, RT, CRT, and IAP were compared by two-way repeated measures ANOVA with treatment and time as independent variables. When a significant difference was found, Tukey's test or paired t-test was applied as appropriate. Sedation and analgesic scores were compared by nonparametric Friedman's test, followed by Wilcoxon signed ranks test. Statistical significance was considered at p < 0.05.
Results
HR and RR significantly decreased from baseline with X and XT treatments, and significantly increased with T treatment (Table 1). A significant decrease in HR was more pronounced with X treatment (from 5~25 min) than XT treatment. RT was significantly increased from baseline with X treatment (from 5~10 min), T treatment (from 10~120 min), and XT treatment (at 75 min). CRT did not change significantly with any treatment. Significant increases in IAP were detected with X and T administered individually, but there was no significant change in IAP noted with XT treatment (Table 2).
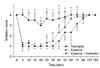
X and XT produced sedation within 5 min, which lasted 50 min for X and 75 min for XT. T treatment induced light sedation only at around 20 min. XT treatment showed a greater sedative effect than X alone (at 40, 60, and 75 min) (Fig. 1).
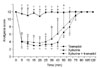
The onset of analgesia was approximately 5 min with both X and XT. Analgesia persisted for 50 min with electrical stimulation and 40 min with pinprick for X, and 60 min for XT. T induced only light analgesia at about 10 min with electrical stimulation. In the assessment of analgesia with electrical stimulation, XT treatment produced a greater analgesic effect than X alone at 60 min, while no statistically significant difference was evident with the pinprick method (Figs. 2 and 3). At the initial phase, XT treatment produced lower, but not statistically significant, sedative and analgesic effects with electrical stimulation than X alone.
During the experiments, complications were observed in horses receiving X (second degree atrioventricular block, salivation, urination, and sweating) and T (muscle tremor, eye blinking rate increase, yawn, chewing, and tongue darting in and out) (Table 3). Horses receiving the XT combination displayed these complications infrequently, although two horses initially displayed signs of sedation and then became excited approximately 3 min after drug administration, with sedation signs reappearing within 5 min. In one of the latter horses, T was accidently administered rapidly (within 2 min). The standard procedure was followed for the other horse.
Discussion
When facilities are limited and/or the physical status of the patient is not suitable for general anesthesia, many surgical procedures can be performed in a standing position with sedation and analgesia. The combination of α2 agonists and opioids are most commonly used in standing horses for painful procedures such as laceration repair, flank laparotomy, and castration [10]. In this study, X and T were evaluated individually and in combination for clinical use in equine practice. X is an extensively studied agent and is more economical to use than other α2 agonists, and T, a potential analgesic opioid in horses, is not a controlled drug in South Korea.
Unlike in humans, assessment of analgesia in animals is difficult [3,5]. Methods used to assess analgesia in horses include skin and deep muscle pinprick, pin pressing on the cannon bone, electrical stimulation to the coronary and/or fetlock region with hoof withdrawal, and skin twitching reflex latency with use of a heat lamp [2-4,12]. Analgesic effects of α2 agonists or opioids can be quantitatively different according to the nociceptive test used [2,4,12]. In this study, electrical stimulation on the left flank region and pinprick on the right neck, flank, and hip regions were used to assess analgesic effects. Results were more apparent with electrical stimulation than with the pinprick method. During the experiment, as the test with pinprick was repeated, horses tended to associate the approach for pinprick with the painful stimulus which may have influenced the analgesic effect results.
IV administration of X provides sedation and analgesia [5,6,9,12,17]; however, the duration and degree of these effects vary according to the drug dosage and evaluation method used. Complications encountered with X may include decreases in HR and RR, initial transient hypertension, wide-based stance, ataxia, second degree atrioventricular block, urination, and sweating. In this study, X produced sedation for 50 min, and analgesia for 50 min (electrical stimulation) and 40 min (pinprick). A previous study reported that the IV administration of 1 mg/kg X produced sedation for 60 min and analgesia for 40 and 60 min as assessed by nociceptive withdrawal reflex and a temporal summation model, respectively [17]. Horses may appear well sedated by α2 agonists, but they can suddenly respond to painful stimulation [5,10]. This response usually cannot be reduced by increasing the dose of α2 agonists, which may pose a danger to both the patient and the attending veterinarian. For these reasons, opioids are commonly combined with α2 agonists to decrease this response.
T is a weak µ-opioid receptor agonist, partially antagonized by the opioid naloxone. It produces analgesia by opioid and nonopioid mechanisms, and acts as an inhibitor of the reuptake of monoamine neurotransmitters such as norepinephrine and serotonin [16,18]. Compared to other µ-receptor agonists such as morphine and codeine, respiratory depression with T is less at the recommended dosage [16,18]. T undergoes extensive metabolism in the liver, where it is converted to various metabolites [18]. In humans, the ratio of hepatic metabolites is affected by cytochrome P450 variations [7,18]. The T O-desmethyltramadol (M1) metabolite has a 200-fold higher affinity for the µ-receptor than the parent drug, and M1 is likely the principle reason for the analgesic effect produced by T [18]. T-mediate analgesia can be produced by provision of very low levels of M1 in horses [8,19]. This may have influenced the present results, given that T produced only mild sedation at 20 min and analgesia at 10 min with electrical stimulation. As previously reported, cumulative (0.1~1.6 mg/kg every 20 min) and single bolus (2 mg/kg) injections of T did not produce sedation and analgesia, but horses tended to adopt a wide-based stance [4].
Intravenous T does not produce locomotor stimulation that has been observed with other opioids, but has been found to create other CNS excitation such as more excited and alert behavior, increased sensitivity to noise and stimulation, trembling, and head nodding [4]. Similarly, in this study, CNS stimulant effects were observed, included muscle tremor, increased rate of eye blinking, yawning, tongue darting in and out, and chewing motion. Increases of HR, RR, and RT may occur secondary to CNS stimulation. Muscle twitching, which as an adverse effect of intravenous T (2 mg/kg), can be alleviated by extending the time of administration to 10 min [19]; therefore, slow IV administration of T may help to minimize other adverse effects.
Despite the lessened sedative and analgesic effects of intravenous T, epidural injection of T has been shown to produce long-lasting analgesia without CNS excitation and changes in motor activity and behavior [13,14].
To our knowledge, this is the first study to examine the clinical effects of a combination of an α2 agonist and T. Although the combination of α2 agonists and other opioids have been extensively studied and are widely used in equine practice, reflecting their increased clinical effects and decreased side effects [3,5,10], in this study, two horses in the XT treatment group became excited for 10~30 sec within 5 min after drug administration. This may have resulted from the CNS stimulation effect of T under sedation with X and warrants further study.
Although IV administration of T alone did not induce significant sedation and analgesia in horses, it enhanced the sedative and analgesic effects of X. The results suggest that the XT combination is useful for sedation and analgesia in horses. Also, it is recommended to carefully monitor patients when using XT in combination, due to the possibility of excitement following administration, especially in the early phase.




 XML Download
XML Download