

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Inflammatory and neoplastic processes are the most common diagnostic findings when evaluating canine nasal diseases, these carry very different prognoses. Endoscopy is a common diagnostic tool used to evaluate the nasal cavity and to target samples [2,4,5,10-16]. In a study in 1990, McCarthy and McDermaid [8] stated that the use of the rhinoscopic technique as part of a complete and well-conducted diagnostic investigation can achieve a correct diagnosis in more than 90% of cases without the help of surgical inspection. Such a high percentage of success, in the opinion of the authors, can only be reached by correlating rhinoscopy with all of the clinical and anamnestic information previously gained, and with the radiographic images in the correct projections [8].
To our knowledge, no study in the literature has looked at the correlation between endoscopic and histopathologic findings in a group of dogs with a final histopathologic diagnosis of either neoplastic or primary inflammatory nasal disease.
In order to evaluate the degree of concordance between endoscopic findings and histological diagnosis, a retrospective study was performed to analyze medical records of 54 dogs which presented with symptoms of chronic nasopharyngeal disease later diagnosed as neoplasia or chronic nasal inflammation, after exclusion of mycosis, protozoal diseases (e.g. ehrlichiosis and leishmaniasis) or foreign body inhalation.
Materials and Methods
Clinical cases
We reviewed medical records of 54 dogs which presented at the Department of Veterinary Clinical Sciences, University of Bologna, between January 1, 2005 and October 1, 2008. Each dog had undergone nasal endoscopy and received a final diagnosis of either chronic inflammatory rhinitis or nasal neoplasia. Chronic symptoms were defined as lasting for more than two months and included nasal discharge (mucoid, mucopurulent, hemorrhagic), sneezing, epistaxis or stertor. Other inclusion criteria were normal findings for complete blood count, serum chemistries, clotting examination (aPTT, PT, D-dimer), urinalysis, regional lymph nodes examination, liver echography, and thoracic radiographs. X-ray examination of nasal cavities was performed in all patients.
Information obtained from the medical records included in the study consisted of signalment, history, clinical signs, results of rhinopharyngeal endoscopy and results of histologic examination of nasal biopsy specimens. An initial diagnosis was recorded by the endoscopist on the basis of rhinoscopy and the results of another test (e.g. X-ray).
Cases of ehrlichiosis and leishmaniasis (diagnosed by serology), fungal disease and foreign body inhalation were excluded. The study included 33 sexually intact males and 21 females (13 sexually intact, eight spayed) aged from 1 to 15 years and of 21 different breeds.
Endoscopic examination
Rhinoscopy was performed in all patients with a double endoscopic technique: a rigid endoscope, for the inspection of the rostral part until the ethmoidal volutes of the nasal cavity (anterograde approach), and a flexible endoscope was inserted orally into the nasopharynx (retrograde approach).
Patients underwent general anaesthesia after intubation and insufflation of the endotracheal cuff. In case of unilateral symptoms, both nostrils were examined and rhinoscopy was first performed in the healthy nostril.
Generally, after orotracheal intubation, the first operative phase to be performed was the retrograde approach with the flexible endoscope, because of frequent bleeding during the anterograde approach when using the rigid endoscope or maneuvering instruments. For the retrograde approach, a 6 mm in diameter and 1,050 mm in length flexible bronchoscope (Pentax EG-1840; Pentax, USA) was used, equipped with an instrumental portal to insert forceps for tissue sampling. During this phase, the animal was positioned in dorsal recumbence to facilitate the insertion and manipulation of the flexible endoscope. To further facilitate the insertion of the endoscope into the rhinopharynx, curve grasping forceps were used to hold and pull forward the soft palate. The flexible endoscope was "J-flexed" and pulled cranially to visualize the choanae. A sample tissue was always performed in presence of masses or mucosal abnormalities. However, because biopsy forceps couldn't be inserted in working channel with the endoscope tip flexed, after endoscopic examination, the scope had to be withdrawn from the rhino-pharynx and the biopsy forceps was inserted prior endoscope tip flexion.
After removal of the flexible endoscope, the patient was positioned in sternal recumbency with the head lifted slightly by a soft support. To facilitate the outflow of the fluids used to irrigate the nasal cavities, the patient was put in the Trendelenburg position. The pharynx was packed with cotton swabs to prevent aspiration of nasal exudates or irrigation fluid.
For the anterograde approach, a rigid endoscope (Karl Storz, Germany) with a diameter of 2.7 mm with a 30° angle and a length of 19 cm was used. The endoscope was inserted inside a cannula of 4 mm diameter with a Luer-lock tap for irrigation with fluids and aspiration of secretions. A 2.5 mm endoscopic forceps was used for biopsy.
After the systematic examination of nasal cavities, 3 or 4 biopsy samples were collected. Bilateral biopsy specimens were collected in both endoscopic phases, even when nasal disease was recognized as unilateral, in order to obtain a histopathological confirmation of unaffected nasal mucosa. Abnormalities recorded during examination included mucosal hyperemia or edema, mucus or blood accumulation, presence of a mass, turbinate atrophy and ulceration.
Histological examination
Biopsy specimens were gently extracted from the forceps and properly oriented on cellulose acetate supports (Endofilters Bioptica, Italy), fixed in 10% buffered formalin, embedded in paraffin, sectioned at 4 µm and stained with haematoxylin and eosin. All the slides were reviewed by the same pathologist.
Inflammation was diagnosed when all biopsies showed stromal infiltration of inflammatory cells; in particular, cases were diagnosed as chronic lymphoplasmacytic rhinitis when lymphocytes and plasma cells were the predominant inflammatory cell components, active lymphoplasmacytic rhinitis when a significant proportion of neutrophils was also evident, and eosinophilic chronic rhinitis if eosinophils were readily evident together with lymphocytes and plasma cells.
Cases matching the diagnosis of tumour were classified according to the World Health Organization criteria [3].
Statistical analysis
A comparison was made between the endoscopic report and the histological diagnosis, which was seen as the gold standard.
The agreement between endoscopy and histology regarding the diagnosis of chronic inflammation or neoplasia was tested by application of Cohen's kappa coefficient. A poor agreement was defined as a K value ≤0.20, a fair agreement as 0.21~0.40, a moderate agreement as 0.41~0.60, a substantial agreement as 0.61~0.80 and a good agreement as >0.80.
The influence of gender on the two classes (inflammatory process vs. neoplastic process) was compared using the Chi-squared test with the data arranged in a 2 × 2 table. The influence of age on the two classes was compared by applying a non-parametric distribution test (Wald Wolfowitz run test), in relation to the non-normal distribution of the variables as analyzed by the Shapiro Wilk's W test.
The dichotomous parameters obtained from anamnesis, clinical examination and endoscopy (presence/absence of nasal discharge, unilateral/bilateral nasal discharge, presence/absence of cough, presence/absence of sneezing, patency/obstruction of nasal cavity, unilateral/bilateral involvement of the nasal cavity, involvement/non-involvement of the rhinopharynx, presence/absence of exudate in the nasal cavity, presence/absence of haemorrhage in the nasal cavity, presence/absence of masses, presence/absence of ulcerate masses) were compared using a logistic regression analysis. Significance was assessed for p<0.05.
Results
The endoscopic examination allowed diagnosis of 29 subjects with suspected inflammation of the nasal cavity and 25 subjects with suspected presence of a neoplastic process; the histological examination provided a diagnosis of inflammation in 36 cases (Table 1) and a diagnosis of neoplasia in 18 cases (Table 2). In particular, all cases diagnosed as cancer by histology were also diagnosed as neoplasia by endoscopy, while seven cases histologically diagnosed as inflammation were misdiagnosed as cancer by endoscopy (Fig. 1).
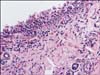
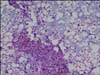
No macroscopic metastases were visualized in regional lymph nodes, lung or liver by x-ray and ultrasound examinations. In the inflammation group, histology demonstrated a chronic lymphoplasmacytic rhinitis in 23 of 36 cases (Figs. 2 and 3), active lymphoplasmacytic rhinitis in 11 of 36 cases, and eosinophilic chronic rhinitis in two cases. Accessory findings in chronic lymphoplasmacytic rhinitis were hyperplasia of the epithelium with areas of squamous metaplasia, excessive mucus secretion and stromal fibrosis. In active lymphoplasmacytic rhinitis there were areas of hyperplastic epithelium with intraepithelial neutrophils admixed with areas where the epithelium was eroded, active fibroplasia of the lamina propria and vasculitis. In eosinophilic chronic rhinitis the epithelium was markedly hyperplastic and infiltrated by eosinophils, and the lamina propria showed vascular proliferation, fibroplasias and accumulation of lymphocytes and plasma cells. As for tumor masses (18 cases), most dogs had epithelial tumors (11 adenocarcinoma and three papilloma) (Fig. 4) and two had malignant mesenchymal tumors (one chondrosarcoma and one liposarcoma) (Fig. 5); furthermore there were one neuroendocrine carcinoma and one mastocytoma.
The seven cases diagnosed as cancer by endoscopy and inflammation by histology were five cases of chronic lymphoplasmacytic rhinitis, one of active lymphoplasmacytic rhinitis and one of eosinophilic chronic rhinitis. In all cases there was marked hyperplasia of subepithelial and epithelial layers which endoscopically matched a tumor-like pattern. In particular, of these seven cases, four were characterized at clinical examination by unilateral nasal discharge, one by bilateral nasal discharge and in two cases by no nasal discharge.
Evaluation of the histological and endoscopic agreement by Cohen's kappa coefficient gave a value of 0.73, indicating a "substantial agreement".
No statistical analysis on the breed was effected in relation with the high dispersion of the sample represented by 21 different breeds.
No significant differences were found when comparing the two groups (inflammation vs. neoplasia) for the variables of gender and age.
Based on the histological diagnosis, the analysis of anamnestic and clinical findings between the two groups showed significantly more frequent unilateral nasal discharge in the neoplasia group than the inflammation group (p<0.01). Meanwhile, no difference was detected between the two groups in terms of presence/absence of nasal discharge, presence/absence of cough and presence/absence of sneezing.
Based on the endoscopic diagnosis, several parameters were significantly more associated with the neoplasia group: the obstruction of the nasal cavity (p<0.001), the unilateral involvement of the nasal cavity (p<0.01), the involvement of the rhinopharynx (p<0.001), the presence of blood in the nasal cavity (p<0.05), and the presence of a mass in the nasal cavity (p<0.001). No differences were detected between the two groups for the presence/absence of an ulcerated mass in nasal cavity or for the presence/absence of an exudate in the nasal cavities.
Discussion
The inspection of the nasal cavities by the anterograde approach with a rigid endoscope (diameter of 2.7 mm) allowed a complete visualization of the ventral meatus only in patients heavier than 10 kg. The inspection in dogs of a smaller size was comparatively difficult and often incomplete due to the instruments and the impossibility of performing some movements mandatory for the visualization of the meatus. In addition, a further factor able to influence the degree of visualization of the nasal cavities seemed to be the morphology of the head. In particular, in brachycephalic dogs the forward endoscopic visualization was more difficult independent of body weight.
Nevertheless, the use of the two different endoscopic approaches (retrograde and anterograde) and the specific endoscopes used in this review decreased the range of unexaminable areas. As previously reported in the literature, an examination with rigid endoscopes precludes visualization of nearly 50% of the caudal portion of the nasal cavity, while a combined approach of anterograde visualization with a rigid endoscope and retrograde visualization with a flexible endoscope provides a broader view of the nasal cavity [17].
In the retrograde approach, the flexible endoscope had to be positioned for the acquisition of only one image, thus the inspection was not hindered no matter how small the dog was. The only limitation with the flexible endoscope was the anatomy of each dog, and depending on the dimensions of the pharynx, it was sometimes more difficult to bend the endoscope backwards to visualize the nasopharynx in smaller subjects.
It should be stressed that other imaging techniques such as CT and MRI are able to examine the nasal cavity and border structures with greater sensitivity than endoscopy. However, the current costs of these modalities limit their routine use [1,10]. Also, chronic rhinopathy symptoms tend to be mild for a prolonged period of time, so anatomical changes are often very evident by the time of clinical presentation.
A further inherent strength of the endoscopic approach is that in addition to being an imaging technique it also allows for precise tissue sampling, and thus histological examination, the gold standard for nasal disease diagnosis. This represents an advantage over CT or MRI, for which sampling is only possible in the presence of osteolysis. However, an important and unique advantage of MRI is its ability to differentiate between tumor types (e.g. sarcoma vs. carcinoma) on account of their intensity on T1-Weighted and T2-Weighted images [1].
The comparison of endoscopic diagnoses with histological results has elicited a substantial agreement (Cohen's kappa coefficient: 0.73). This value was reached with the acquisition of several biopsy samples (at least four) during the endoscopic examination and with the continued cooperation and interchange of information between the clinicians and the pathologist.
Chronic idiopathic inflammatory rhinitis is generally characterized by a primarily lymphoplasmacytic infiltrate or, less frequently, by a concurrent neutrophilic and eosinophilic infiltrate [18]. This condition was present in our study with 23 of 36 cases characterized by an infiltrate of lymphocyte and plasma cells, 11 of 36 cases with prevalent neutrophilic and plasma cell infiltrate, and 2 of 36 with prevalent infiltrate represented by eosinophils and plasma cells. It is difficult to affirm if the neutrophilic/eosinophilic infiltrate represents an evolution of the process started with lymphocyte and plasma cell reaction or a response to a different inflammatory stimulus.
The prevalence of nasal tumor in the literature ranges between 0.3% and 2.4% of all neoplasia surveyed in the dog, with a high incidence of carcinomas (particularly adenocarcinomas and squamous cell carcinomas) which metastasize, rarely, to the brain, lymph node, lung and liver. Lower incidence is represented by sarcomas (fibrosarcoma, chondrosarcoma, osteosarcoma and undifferenciate sarcoma) [9]. The incidence of the various tumors observed in our study does not differ from what was previously reported in the literature [9]. Indeed, 67% of cancer was represented by carcinomas (adenocarcinoma and neuroendocrine carcinoma) while the remainder consisted of sarcomas, mastocytoma and papillomas. No metastases occurred in regional lymph nodes, lung or liver.
The incidence of breed, sex and age in the development of inflammatory rhinitis compared to nasal neoplasia has been studied by various authors [6,18]. Large-breed dogs have a higher risk in the development of both conditions. A higher predilection in the development of nasal neoplasia has been observed in males, while no gender influence has been proved in dogs with lymphoplasmacytic rhinitis. Similarly the mean age in dogs with nasal neoplasia is ten years [6] and eight years in those with lymphoplasmacytic rhinitis [18].
Accurate statistical analysis regarding the influence of breed on the development of inflammation or nasal neoplasia is limited by the relatively low number of cases involved (n = 54) and the high distribution of breeds. Additionally, almost half the population (n = 25) was represented by mixed breeds.
It should be stressed that no difference was seen between groups in terms of gender and age.
Additionally, the comparison of anamnestic elements and clinical and endoscopic findings in dogs with histological diagnoses of inflammatory rhinitis and nasal neoplasia showed a higher prevalence of unilateral nasal discharge in the neoplastic group, associated with unilateral nasal cavity involvement, the obstruction of the nasal cavity, the evidence of a mass in the nasal cavity, the involvement of the rhinopharynx and the presence of blood in the nasal cavity. Our results contrast with those of a study on canine nasal and paranasal tumors by Ogilvie and LaRue [9] evidencing a bilateral dissemination of nasal neoplasia in almost half of the analyzed cases.
Windsor et al. [18] reported that in course of lymphoplasmocytic rhinitis, nasal discharge was unilateral in 42% and bilateral in 58%. However, there was no agreement between clinical and endoscopic examination, with the latter evidencing a unilateral involvement in 11% and bilateral involvement in 89%.
Similarly, in our study, while the clinical examination evidenced unilateral nasal discharge in the course of chronic inflammatory rhinitis in 39% of cases and bilateral discharge in 61%, less variability was seen on endoscopic examination, with 32% unilateral involvement and 68% bilateral involvement. Other clinical symptoms, namely nasal discharge (unilateral or bilateral), cough or sneezing and the presence of exudate inside the nasal cavity, seemed to be equally associated with inflammatory and neoplastic nasal disease, in agreement with the literature [7,9].
No lymph nodes or pulmonary metastases were seen at the time of neoplasia diagnosis, in agreement with Ogilvie and LaRue [9] who only found metastasis (commonly in the brain, lymph nodes, lung and liver) later in the course of the disease.
In conclusion, rhinoscopy, while superficial in nature, combines good quality diagnostic investigation with the possibility of operative procedures, reducing invasiveness and the time under anaesthesia, and consequently improving the safety of the patient. Moreover, the combined rhinoscopic technique allows a complete exploration of the nasal cavity, the observation of macroscopic images useful for the pathologist, and the advantage of being able to perform several biopsies. It is important to note the advantage of imaging magnification which, like other endoscopic techniques, allows greater inspection of the nasal internal surface, even if it is sometimes not enough to visualize microscopic lesions.
Finally, it is our opinion that different sites have to be always sampled, to avoid the error of withdrawing inadequately or achieving bad processing samples.





 XML Download
XML Download