

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Allotransplantation is currently viewed as the preferred solution for the treatment of end-stage organ failure. However, only a small percentage of those patients who could benefit from this therapy receive it due to a shortage of donor organs [8,21]. This shortage of donors has stimulated interest in the possible use of animal organs for transplantation into humans. Animal-to-human transplantation (or xenotransplantation) would offer an increasing supply of organs and tissue for transplantation. Xenotransplantation using pig organs could solve the significant increasing shortage of donor organs for allotransplantation due to the anatomical and physiological similarities between pig and human organs [7].
In comparison to other solid organ transplants, there have been few reports regarding lung xenotransplantation between pigs and other non-human primates [4,18]. A previous study reported excellent respiratory function and adequate hemodynamics during the short survival time of xenogeneically perfused porcine lungs [6]. In addition, it has been reported that the transplanted pig lungs into cynomolgus monkeys had adequate function [17]. These results suggest that porcine lungs are physiologically compatible with those of humans, although it would appear that pulmonary xenotransplantation is limited by hyperacute lung injury [25].
In order to transplant swine lungs into humans, physiological and anatomical comparison and analysis are essential in assessing the suitability of donor organs for potential recipients. However, an appropriate method for evaluating micropig organs has yet to be established. This study examines the feasibility of evaluating the lung and its related structures using multi-detector row computed tomography (MDCT) and establishes standard anatomical reference values for micropig lungs. Of the major technological developments in computed tomography in recent years, the most significant has been the introduction of MDCT, which has brought about substantial improvements in spatial and particularly temporal resolution [10,13]. This study is the first to show MDCT to be a reliable method for noninvasively assessing the pulmonary anatomy of micropigs.
Materials and Methods
Animals
The micropigs were purchased from PWG Genetics Korea (Korea). Prior to purchase, physical examinations were performed and their results were considered to be normal. The animals were kept in individual cages at the central animal facility and received a standard pig meal and water ad libitum. Six Yucatan micropigs with no clinical evidence of airway or lung disease were selected. All micropigs used in this study were male. The mean age and weight of the micropigs were 360 days and 30.50 ± 1.24 kg, respectively. Permission to perform this study was obtained from the Ethics Committee of Chonnam National University (CNU IACUC-YB-2008-29). Before the CT imaging procedures, all animals were fasted for a minimum of 24 h. The animals were premedicated by an intramuscular injection of azaperone (0.5 mg/kg) and xylazine (8 mg/kg), and anesthetized with an intramuscular injection of a combination of zolazepam/tiletamine (4.4 mg/kg).
Image acquisition using MDCT
All animals underwent CT imaging with a 64-channel multi-detector row helical CT scanner (Lightspeed VCT; GE Healthcare, USA). The CT angiographic scan was obtained in the craniocaudal direction. The acquisition parameters for 64-MDCT were 120 kVp; reference tube current of 140~200 mAs, collimation dimension of 5 mm, rotation time of 0.5 second, 1.0 pitch, reconstruction thickness of 1 mm, and a reconstruction increment of 0.5 mm.
For administration of intravenous contrast material, a 20-gauge peripheral line was inserted into an ear vein. After a scout CT image was obtained, arterial phase volumetric image data sets were acquired after the start of an intravenous injection of 60 mL of a nonionic contrast media (Ultravist 370; Schering AG, Germany) at an injection rate of 3 mL/sec using an automated injector (LF CT 9000; Liebel-Flarsheim, USA). The automatic bolus triggering software program was systematically applied, with a circular region of interest (ROI) positioned at the level of the superior vena cava and a threshold for triggering data acquisition preset at 100 HU. MDCT scanning was obtained from the thoracic inlet to the diaphragm. All scanning was performed during normal respiration, without suspended breath holding. The volumetric data sets were then transferred to a workstation (GE Advantage Workstation 4.3; GE Healthcare, USA) that runs 3D software (Volume Viewer Plus; GE Healthcare, USA) for subsequent review. Transverse 0.625-mm-thick sections were reformatted into maximum intensity projection images and volume rendered images.
Image analysis
One radiologist reviewed all CT studies. All images were reviewed on a workstation which allows the reviewer to edit CT volume data sets to create optimal three dimensional (3D) CT angiography images and images of central airways in real time. The 3D reconstruction images were reviewed in conjunction with the review of the conventional 2D axial images. The CT angiographic images were reviewed by scrolling the acquisition displayed on a workstation monitor.
For the evaluation of tracheobronchial tree, 2D multiplanar reformation images along the axis of the trachea and 3D external images of central airways were obtained. The reviewer measured the diameter of the distal trachea just proximal to the bifurcation and that of each main bronchus just distal to the bifurcation on a workstation. An electronic cursor was used to measure the widest diameter perpendicular to the long axis of the distal trachea and each main bronchus.
For 3D CT angiography, volume-rendering techniques were usually used, but maximum-intensity-projection rendering was also used as an adjunct display. Pulmonary arterial and venous anatomies were evaluated on arterial phase images. After 3D CT images of the pulmonary vessels were obtained, the reviewer recorded the branching pattern and the diameters of each pulmonary artery. An electronic cursor was used to measure the widest diameter perpendicular to the long axis of the main pulmonary artery, right pulmonary artery, and left pulmonary artery at the pulmonary artery bifurcation level. Pulmonary vein anatomy was evaluated for the number and diameters of the pulmonary veins and the presence of any anatomic variations. The reviewer measured the diameters of the most proximal portion of the right or left superior pulmonary vein and right or left inferior pulmonary vein by using an electronic cursor on a workstation.
The lung volume was measured from contiguous slices. In coronal reformatted images, the region of interest was drawn around the lung, and the slices were reconstructed at 1-mm intervals to obtain a 3D volume-rendered image of the lung. The volume was calculated by multiplying the sum of areas from each slice by the reconstruction interval.
Results
The MDCT examinations were technically satisfactory in all animals. High quality 2D multiplanar reformatted images and 3D reconstruction images of central airways were obtained in all animals (Fig. 1A). The mean diameters of distal trachea, right main bronchus, and left main bronchus were 1.06 ± 0.17 cm, 1.18 ± 0.14 cm, and 1.1 ± 0.11 cm, respectively. A tracheal bronchus to the right upper lobe was noted in all micropigs (Fig. 1B). No stenosis or endoluminal lesion in central airways was noted in all micropigs.
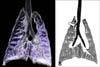
3D volume rendering CT angiographic images of pulmonary vessels were obtained in all animals (Fig. 2). The mean diameters of the main pulmonary artery, right pulmonary artery, and left pulmonary artery were 1.38 ± 0.09 cm, 1.07 ± 0.26 cm, and 0.98 ± 0.13 cm. The branching pattern of the main pulmonary artery was similar to the human anatomy. There were no anatomic variations in the major pulmonary arteries of all micropigs.
The anatomical structure of the pulmonary veins was different to that seen in humans. There were a single venous trunk, the common inferior pulmonary vein, which drains both the right and the common inferior pulmonary vein in all micropigs (Fig. 3). Both right and left superior pulmonary veins directly drained into the left atrium. The mean diameters of the right and left pulmonary veins were 0.97 ± 0.20 cm and 0.76 ± 0.20 cm, respectively. The mean diameter of the common inferior pulmonary venous trunk was 1.99 ± 0.26 cm.
The mean volume of the lung was 820.3 ± 77.11 mL. MDCT depicted no abnormalities of the pulmonary parenchyma in all micropigs. The clinical and radiographic data on the pulmonary systems of the 6 micropigs are summarized in Table 1. Furthermore, when compared the mean diameter of trachea, main bronchus, pulmonary artery and vein, considerable difference was apparent between human and micropigs. The mean diameter of main pulmonary artery in micropigs was about 51.9% of that of human (Table 2).
Discussion
This study was performed to establish the standard anatomical reference values of micropig lung and to examine the feasibility of 3D MDCT as a method of assessing the complex pulmonary anatomy in order to improve micropig lung donor selection and surgical planning. In order to transplant swine lungs into humans, the anatomical and physiological differences between donors and recipients need to be analyzed and determined. In previous reports, xenotransplantation of pig lungs was limited due to the severe vasoconstriction occurring in the newly transplanted lung [19], but the pig lung has been demonstrated to provide adequate oxygenation and carbon dioxide exchange in the non human primate [6]. In this study, we measured the anatomical, volumetric, and vascular parameters of micropig lungs using 64-channel MDCT. The mean airway and pulmonary vein diameters, and the branching pattern of the pulmonary artery were similar to those of humans. Furthermore, there was no stenosis or endoluminal lesions in central airways, further indicating the suitability of micropigs may as lung donors. Despite the considerable similarities in the pulmonary anatomies of humans and micropigs, however, there are differences in the diameter of the main pulmonary artery. These differences indicate the possibility that the function of micropig lung in gas exchange is less than that of the human lung. Thus, further studies to compare micropig and human lung ventilation and perfusion are needed.
For lung transplants, preoperative evaluation of donor anatomy allows surgeons to determine which potential donors to use for lung donation, and which to decline, as there is considerable complexity and variation in pulmonary venous anatomy. In light of the even greater anatomical differences between humans and micropigs, it will therefore be especially important to establish preoperative evaluation and selection guidelines for micropig donor lungs.
Chest CT scans have been routinely performed in potential donors to exclude pulmonary parenchymal pathology and estimate lung volumes [2,5,24]. Preoperative knowledge of the pulmonary anatomy is necessary for lung transplantation, but it is undesirable to subject donors to invasive catheterization [1], and the use of a minimally invasive means of delineating precise pulmonary anatomy was requested in order to identify donors with the most favorable arterial anatomy. Over the past few years, MDCT has been used for noninvasive pulmonary imaging, as MDCT angiography is highly accurate for the evaluation of pulmonary structure and function [7,11]. The advantages of MDCT are faster image acquisition, improved image resolution, and superior contrast reinforcement [9,14]. In addition, MDCT not only provides anatomic information, but is also used as a pathologic or diagnostic tool [15]. Furthermore, the number of detectors has gradually increased since the introduction of MDCT in the early 1990s [20], with 64-channel MDCTs generally used for human clinical use at present. Increasing the number of detectors allows for good quality images, even in moving organs such as heart and lung, through improvement of spatial and temporal resolutions [3].
In the present study, we evaluated pulmonary anatomic parameters including lung volume, direction of pulmonary blood flow, and the diameters of trachea, bronchus, arteries and veins by MDCT. We also observed that the right and the left inferior pulmonary veins form a common trunk which drains into the left atrium in micropigs. In humans, it is known that the right and left inferior pulmonary veins separately drain into the left atrium. Although these observations are already well known in comparative veterinary anatomy, MDCT can also provide useful indicators of the normality of the organ, such as airway lumen and wall segmentation, parenchymal density or texture, quantification of regional ventilation and perfusion parameters, occurrence of various pulmonary diseases [11]. Therefore, MDCT is an appropriate method to determine the normality and suitability of donor lungs for transplantation.
In conclusion, 64-channel MDCT imaging provided morphological details and spatial resolution data of the lung and understanding of pulmonary vasculature in micropigs.




 XML Download
XML Download