

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Multilobular tumour of bone (MTB) is an uncommon tumour that typically affects the canine skull, usually presenting as a firm, circumscribed and generally slow-growing bone tumour in older dogs from medium or large breeds. Its biological behaviour may range from benign to malignant, with the potential to invade, metastasise and recur [16]. Histologically, it is characterised by the dominant presence of multiple osteoid- or cartilage-containing lobules that are separated by fibrous septae [15]. Although most frequently found in dogs, MTB has been reported in humans [5], cats [5], a horse and a ferret [3]. The clinical signs depend on the tumour location and aggressiveness, and may include neurological or ocular signs and disfiguration of the face [2,17]. Depending on its location and stage in the clinical course, aggressive surgical resection may result in long-term remission [2]. The literature regarding MTB is limited to a relatively small number of case reports and a single review of 39 cases [2], expanded from an earlier review of 16 cases [16]. In these studies, the tumour has been reported to most commonly involve the mandible [13], maxilla or the calvarium [2,11], and occasionally other sites such as the orbit [11], hard palate [1] and zygomatic arch [2]. Previously, a small number of tumours specifically arising from the occipital bone have been reported [4]. To our knowledge, the present report is the first of an MTB arising from the external occipital protuberance and causing severe compression to both the cerebrum and the cerebellum.
A 13 year-old male mixed breed dog was presented with a two-week history of progressively worsening signs of vestibular dysfunction that were further aggravated with severe cognitive abnormalities. Upon neurological examination, the animal appeared demented and showed a left head tilt, asymmetric ataxia and hypermetria. Postural reactions were abnormal on the left side, whereas spinal reflexes were present (+2) in all four limbs. Following the neuroanatomical localisation of the lesion to the medulla (left cerebellopontine angle), a preliminary clinical diagnosis of structural encephalopathy (neoplastic or inflammatory) was offered. The perceived grave prognosis led the owner to refuse pursuing further diagnostic investigations and opted to have the animal euthanised.
Necropsy revealed the presence of a spherical, mostly well-circumscribed mass approximately 6 cm in diameter concerning the right occipital, parietal and temporal bones and protruding from the right occipital bone (Figs. 1A and B). The mass severely compressed the cerebellum and the right occipital lobe (Figs. 1C and D) but did not appear to invade the brain tissue, the meninges or other neighbouring tissues. The mass was whitish to yellow and gritty on the cut surface. The lungs were congested, haemorrhagic and had scattered depositions of black pigments, consistent with anthracosis. There was no evidence of palpable or macroscopically visible metastatic foci. The liver was severely congested.
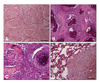
Histologically, the tumour was characterised by the presence of multiple lobules containing osteoid or cartilage in the center that were separated by anastomosing fibrous septae (Figs. 2A and B). Similar to its macroscopic appearance, there was no evidence of the tumour invading into the neighbouring tissues. Overall, the tumour was well-differentiated. Most lobules were small to medium in size and round or oval. The lobules contained cartilage, osteoid or bone in their centers and were with or without chondrocytes or osteocytes in their lacunae. Also, the lobules had a variably sized layer of chondroblasts or osteoblasts, surrounded by a thin fibrous septum, both oriented radially around the matrix-containing center.
In general, the lobules containing cartilage were larger than the osteoid-containing ones. The lobules of the cartilage-containing tumors were well organised and clearly defined. Their mitotic index was low, with less than one mitotic cell per high power field. Necrotic areas covered 10-15% of the examined area, and mainly concerned the cartilage-producing areas. In one marginal large area of the tumour, the lobules were not as well formed or defined, and the tumour cells were arranged in sheets, or otherwise exhibiting cellular features denoting a high-grade malignancy (Fig. 2C) reminiscent of osteosarcoma. Osteoblast-like cells were moderately pleomorphic, often having vesiculated nuclei and prominent nucleoli, although the mitotic index was low. Both osteoid- and cartilage-containing lobules were observed in these areas.
Small metastatic foci were present in the lungs. Some degree of histological similarity to the primary site was retained and the multilobular pattern was still clearly evident. Tumour lobules of these foci were smaller and more uniform in size, contained mainly chondroid tissue in the center and had thinner fibrous septae (Fig. 2D). The mitotic index of these foci was low and small necrotic foci were present in the center of the larger metastatic foci. Based on the above, a diagnosis of a malignant MTB of the occipital bone with lung metastases was established and the tumour was classified as Grade I [16].
This report describes in detail an MTB affecting the caudal cranium and causing severe cerebral and cerebellar compression. In the only large series to date describing the clinical features of 39 cases [2], none of the cases concerned the occipital, parietal or temporal bones as in the case presented here. A small number of tumours specifically arising from the occipital bone have been reported previously [4,7]. In these cases, the mass compressed, without invading, the cerebellum and brainstem but did not affect the cerebrum [8]. Two cases affecting the calvarium, treated with cranioplasty after en bloc resection of the tumour, had good clinical course post-surgery and, unlike the present case, did not develop metastases [12]. In another case, a tumour located at the dorsum of the head developed metastases [9]. The only other case of MTB arising from the occipital bone described in detail [7] indicates that it arose from the internal occipital protuberance, and affected the cerebellar meninges and the cerebellum without causing cerebral compression.
MTB should be included in the differential diagnosis of bone tumours concerning the canine skull; there are substantial differences in the progression of the disease, metastatic incidence and median survival time between tumour entities and conditions affecting bone [14], establishing, therefore, the correct diagnosis alters the prognosis and is paramount in pursuing the optimal therapeutic protocol. Most bone tumours are osteosarcomas, and MTBs may be misdiagnosed as such [10]; however MTB must also be differentiated from other primary bone tumours, particularly chondrosarcoma [6,10]. Other, non- neoplastic causes of neurological signs associated with cerebral and cerebellar dysfunction should be ruled out in these cases, employing, when feasible, advanced diagnostic imaging or other techniques.
There has been a certain degree of confusion in the veterinary literature concerning MTB, due to its rarity, varying biological behaviour and varying levels of matrix production that may include osteoid tissue, bone or/and cartilage. A number of terms have been used in the literature in the past as synonymous to MTB in various species, including chondroma rodens, cartilage analogue of fibromatosis, calcifying aponeurotic fibroma, juvenile aponeurotic fibroma, multilobular osteoma, multilobular chondroma, multilobular osteosarcoma and multilobular osteochondrosarcoma [3,16]. The entity is now almost universally termed multilobular tumour of bone, a term that takes into account the characteristic histologic features of the tumour and does not refer to its behaviour that can be benign or malignant.
Although the case was histologically categorised as a low grade malignancy, it exhibited biological features of a high grade malignancy, as it metastasised to the lungs and caused extremely severe cerebral and cerebellar compression that led to severe subacute neurological dysfunction. The metastatic foci of the present case were few and small in size; a radiological examination may not have revealed their presence. In any case, the decision to euthanise the animal was taken on the basis of the severe neurological signs, particularly the progressively worsening cognitive and locomotor dysfunction. Importantly, MTBs located in the skull are not always accompanied by neurological signs, and when they are, they are not necessarily severe [8]. Given the extent of cranial vault invasion and the fact that a large portion of the tumour was located intracranially, it is uncertain whether performing a partial craniectomy would be feasible and whether it would help alleviate the dog's symptoms.
The majority of reports on MTB originate from the USA, with only a small number of cases having been reported from other countries [12]. Although most aspects of the disease have been described in the aforementioned reports, its histogenesis and pathogenesis remain unclear. The cranium is a complex of bones formed in both membrane and cartilage; the multilobular cartilage- and bone-containing morphology of the tumour may imply embryonic cartilage ossification or periosteal origin, a hypothesis that will require further investigation, together with efforts to detect the genomic or genetic alterations that are implicated in its initiation and progression.

 XML Download
XML Download