

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Intervertebral disc disease (IVDD) is one of the most common causes of neurologic dysfunction and debilitation in dogs, especially Dachshunds and other chondrodystrophoid breeds [17,31,36]. In our hospital, IVDD accounts for approximately 200 cases each year. Surgical removal of extruded disc material is the most commonly recommended treatment for dogs with chronic or recurrent clinical signs, paraplegia, and/or severe back pain [7,19,31,34]. Rapid and accurate pre-operative localization of the extruded disc material is important for minimizing anesthesia-related hypotension and further reduction of spinal cord blood flow, minimizing the time required for surgical exposure, minimizing surgical manipulation injury of the spinal cord, and maximizing complete removal of disc fragments [34]. Complete removal of disc fragments from the vertebral canal is important for minimizing post-operative morbidity due to local inflammatory reactions and persistent spinal cord compression [12,13,26]. Neurologic examination and survey radiography are helpful as preliminary screening tools for dogs with suspected disc extrusion, but these techniques have a low accuracy for predicting the location, extent and side of disc material relative to surgical landmarks [4,18,20,34,35].
Computed tomography (CT) is a sectional imaging technique that is currently available at most veterinary referral centers and is becoming increasingly available at veterinary primary care centers [24]. Computed tomography has been previously validated as a sensitive, non-invasive method for pre-operative diagnosis of acute thoracolumbar disc extrusions in dogs [25]. In a recently published study, the diagnostic sensitivity for CT was found to be similar to that of myelography [15]. Advantages of CT for evaluating canine disc extrusions include elimination of superimposition, fast image acquisition, and low risk of morbidity due to procedure-related complications. However, accurate assessments of spinal lesion localization, extent of involvement, and anatomic landmarks can sometimes be difficult to determine from transverse, two-dimensional (2D) images [29,30]. Angulation or curvature of the spine may cause some transverse slices to be oriented at an oblique angle relative to the long axis of the vertebral canal. Oblique orientation of the transverse slices, even if mild, can distort the appearance of anatomic structures and make it difficult for surgeons to assess affected sides, extent, and severity of vertebral canal involvement. Gradual changes in vertebral canal or spinal cord opacity can also be difficult to detect using sequential viewing of 2D images.
Image post-processing (reformatting) software can be used to convert a set of 2D CT slice images into a set of volume data for interactive manipulation and visualization [5]. Reformatting software is a standard feature of most newer-generation CT scanner computers and is also available for purchase (e-Film; Merge Healthcare, USA) or via the Internet as a free download (OsiriX for Macintosh; ImageJ for Macintosh, Windows, and Linux systems). Spinal angulation can be corrected using oblique multi-planar reformatting (MPR) software tools. Spinal curvature can be corrected using curved MPR software tools. Previous studies have demonstrated the utility of MPR CT images for evaluation of human spinal diseases [2,21,23,27-30,32, 33]. To our knowledge, no controlled studies have described the utility of MPR CT images for assessment of canine IVDD. The purpose of this study was to test the effects of MPR CT on surgeon diagnostic performance in a group of dogs with confirmed thoracolumbar intervertebral disc extrusions. We hypothesized that surgeon diagnostic accuracy, diagnostic certainty, and inter-observer agreement would be improved for MPR CT images versus 2D CT images.
Materials and Methods
Case selection
This study included 111 client-owned dogs that had undergone CT imaging and surgery to treat thoracolumbar intervertebral disc extrusion(s) and secondary myelopathy at the Virginia-Maryland Regional College of Veterinary Medicine between May 2005 and September 2006. Animals were included if 2D and MPR CT image file sets were available in the hospital's digital image archive and if a compressive myelopathy secondary to extruded disc material within the vertebral canal had been confirmed at surgery. Dogs who had myelographic contrast injections prior to CT image acquisition were excluded. Dogs who had previous thoracolumbar surgery were also excluded.
Medical records review
The first author reviewed medical records and recorded clinical data for each dog. Information recorded from the medical records included the patient name, signalment, body weight on the date of surgery, and the complete surgical report from that visit. Data recorded from the surgical report included the surgical diagnosis, surgical site (disc space), and the side (left, right, bilateral, or mixed) on which disc material was found.
CT scanning and reformatting techniques
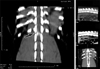
All 2D transverse CT images were acquired using the same single detector spiral CT scanner (Picker PQ5000; Universal Medical Systems, USA). Dogs were placed under general anesthesia and positioned in dorsal recumbency. The standard scanning protocol consisted of transverse slices from mid-T10 to mid-L3 [25]. Additional slices were obtained if requested by the primary care clinician or duty radiologist. Slice thickness settings ranged from 2~3 mm, with a 1 mm slice overlap. Two-dimensional CT image sets for each dog were converted into Digital Imaging and Communications in Medicine (DICOM) format and transferred via Ethernet to a Picture Archiving and Communication System (PACS) (RapidStudy; Eklin Medical Systems, USA). Immediately after scanning, studies were also transferred via Ethernet to a CT workstation (Voxel Q Visualization Station; Picker/Philips Medical Systems, USA). Multi-planar reformatted CT images for each dog were created by the on-duty radiologist, using the workstation's image analysis software. Oblique transverse MPR images were generated using the oblique MPR tool, with the slice angle oriented perpendicular to the long axis of the vertebral canal (Fig. 1). Oblique sagittal MPR images were generated using the same tool, with the slice angle oriented parallel to the long axis of the vertebral canal (Fig. 2). Curved dorsal MPR images were created using the curved MPR tool, with a hand-traced line of cut along the dorsal margins of vertebrae (Fig. 3). Each MPR image was saved as a screen capture and the set of saved images was transferred to the PACS via Ethernet. The MPR image set was stored in the PACS as a separate file for each dog, with the identifier "screen save" included in the file name.
CT image review
Two board-certified veterinary surgeons and one board-certified veterinary neurologist independently reviewed the digital CT image sets for each included dog. Readers were unaware of clinical and surgical findings at the time of review. Readers retrieved CT image sets from the PACS using an in-hospital network and reviewed images at a diagnostic workstation using standard DICOM viewing software (e-Film; Merge Healthcare, USA). Each reader reviewed 2D CT image sets first, with the list of cases arranged in random order. After they had completed review of 2D CT images, readers were then given a re-randomized list of cases and asked to review MPR CT image sets. Readers recorded their opinions using questionnaires. One questionnaire was created for each of the 2D CT file sets and a separate questionnaire was created for each of the MPR file sets. In the 2D CT questionnaire, readers were asked to record their localization of the extruded disc material and their prediction for which side was affected (left, right, bilateral, or mixed). The questionnaires allowed the participants to write in their lesion localization free hand. Participants were instructed to be as descriptive as possible concerning the site and extent of the extruded disc material. Readers used a numerical rating system (1~10) to indicate their certainty for each diagnosis. For the MPR CT questionnaires, readers were asked to record the same data as above. They were also asked to record which MPR views were available, using the following designations: oblique transverse, curved dorsal planar, sagittal planar, or other. For the available views, readers were asked to choose which they found to be the most helpful in making the diagnosis. An area for general comments was also provided at the end of the questionnaire so that readers could note any other factors that they felt affected their decision-making.
Determination of correct CT localizations
The first author compared CT localizations recorded on reader questionnaires with surgical localizations recorded in medical records. Lesions found in the region extending from the caudal 1/4 of the cranial vertebra to the cranial 1/4 of the caudal vertebra were defined as being located over an intervertebral disc space (Fig. 4). Lesions found in the middle 1/2 of the vertebral body were defined as being located over a vertebra. The site of each lesion was assigned to an arbitrary numbering system that was used for statistical analyses (Fig. 5). Starting at the T8-T9 disc space and ending with the L7-S1 disc space, a number from 1~13 was assigned to each adjacent disc space. Lesions located over vertebral bodies were assigned the cranial disc space's number and a 0.5 value. A reader's localization for CT lesion site was defined as "correct" if at least one of the sites identified by the reader was also identified in the surgical report. A reader's CT localization for lesion extent of involvement was defined as "correct" if it agreed with the cranio-caudal extent of the lesion described in the surgical report. No distinction was made if the reader identified more or fewer lesion sites than those reported at surgery. The reader's CT localization for the affected side (left, right, bilateral, mixed) was defined as "correct" if it agreed with the affected side in the surgical report.
Statistical analysis
A statistician selected and performed all analyses using statistical analysis software (SAS version 9.1.3; SAS, USA). Reader diagnostic accuracy ("correct" or true positive fraction) estimates for 2D CT images were compared to diagnostic accuracy estimates for MPR CT images using Generalized Estimating Equations. Mean certainty scores for 2D and MPR CT images were compared using a paired Student's t-test, after verifying that the paired differences were normally distributed. Only the "correct" reader responses were used for the certainty comparisons. Kappa statistics were used to assess agreement among readers for 2D versus MPR CT images. The frequencies with which MPR views were chosen as "most useful" were compared using Exact Chi-square statistics. For all analyses, a value of p ≤ 0.05 was considered significant.
Results
Signalment
The patient population consisted of 60 males, of which 43 were castrated and 17 were intact. There were 51 females within the group, and 45 of those patients were spayed while six were intact. The Dachshund was the most common breed in the study population, with 63 individuals included. Mixed breed dogs were the second most common, with 16 individuals. Other breeds included the Beagle (8), Pekingnese (3), Shih Tzu (3), Basset hound (2), Cockapoo (2), Jack Russel Terrier (2), Lhasa Apso (2), Poodle (2), Cocker Spaniel (1), Bichon Frise (1), Papillon (1), Peekapoo (1), Rat Terrier (1), Tibetan Spaniel (1), and Wheaton Terrier (1). There was also one German Shepherd Dog that met the inclusion criteria. Patient ages ranged from one year and two months to 11 years and eight months. The average age of the animals included in the study was five years three months, and the median age was six years seven months. The average body weight at the time of surgery was 9.1 kg, with a range of 2.7 kg to 36.8 kg.
Surgical findings
A total of 137 disc extrusion sites were confirmed at surgery in these 111 dogs. In all cases, a hemi-laminectomy was performed to decompress the spinal cord. The vertebral column was approached from the left in 61 cases, from the right in 47 cases, and a bilateral approach was made in three cases. The most commonly affected site in our study population was T12-T13 (40/137, 30%). The thoracolumbar junction was the second most commonly affected site (31/137, 23%). Other intervertebral disc spaces that were frequently encountered in this study were T11-T12 (20/137, 15%), L1-L2 (13/137, 9%), L2-L3 (12/137, 9%). Less frequently affected sites included L3-L4 (6/137, 4%), L5-L6 (4/137, 3%), L4-L5 (3/137, 2%), and L6-L7 (2/137, 1%). Two disc extrusions were present exclusively over the vertebral body. One of these lesions was at the L2 vertebrae and the other was at L4.
Reader diagnostic accuracy and certainty
With 2D CT, the total number of true positive localizations were 102 for reader 1, 104 for reader 2, and 99 for reader 3. With MPR CT, the true positive localizations were 100 for reader 1, 105 for reader 2, and 106 for reader 3. Diagnostic accuracy for identifying the correct lesion site was significantly greater with MPR vs. 2D CT images in one reader (Table 1). A significant increase in mean diagnostic certainty scores was seen in two of the readers for MPR vs. 2D CT images (Fig. 5). Mean diagnostic certainty scores for correct diagnoses were increased from 3~11% with MPR CT images. For all other comparisons, no significant differences were identified.
Inter-observer agreement
A trend for increased inter-observer agreement was seen for MPR vs. 2D CT images (Table 2). However the increase was not statistically significant. Agreement among readers was highest for the 'affected site' and lowest for the 'number affected'. The change in agreement between 2D and MPR images differed from zero for all analyses (site, side, number affected) among all three readers (p ≤ 0.05).
Reader preferred views
Oblique transverse and curved dorsal MPR views were rated most helpful with the highest frequency (Table 3). Two readers preferred the curved dorsal MPR images by a large margin compared to other views. The third reader chose the oblique transverse MPR view more often than any other. Oblique sagittal MPR views were infrequently chosen as most helpful by any of the readers.
Other factors affecting surgeon decision-making
One of the most commonly recorded limiting factors was a difficulty in visually distinguishing between hemorrhage and extruded disc material. Another factor often mentioned was the presence of an abnormal rib number. Other difficulties recorded by readers included: distinguishing chronic disc protrusion versus extrusion, subjectively interpreting the severity of spinal cord compression when multiple non-contiguous sites were suspected, and making accurate localizations when there were abnormal numbers of lumbar vertebrae. Difficulty identifying the right/left radiographic marker in MPR images was also mentioned. Most readers commented that more time was required to interpret 2D CT images versus MPR images, however interpretation times were not recorded.
Discussion
Intervertebral disc degeneration is a biochemically-based aging change that occurs normally in dogs and humans [3,9-11,37,38]. With age, the embryonic notochordal matrix of the nucleus pulposus transforms into a more mature fibrocartilaginous tissue. The primary biochemical change is a decline in chondroitin sulphates and replacement by keratosulfates. This aging change may be accelerated in dogs with chondrodystrophy or mechanical stress-induced changes in the extracellular matrix. In dogs with chondroid disc degeneration, especially Dachshunds, the nucleus pulposus often becomes calcified in situ and extrudes into the vertebral canal through small tears in the annulus fibrosus [16]. Chronically extruded disc material in the vertebral canal can become increasingly calcified over time. Calcified intervertebral disc extrusions most commonly occur in small-breed, chondrodystrophoid dogs, but also have been reported in large-breed, non-chondrodystrophoid dogs [6,22].
Computed tomography is similar to radiography in that visualization of structures is dependent on variations in tissue physical density and the associated differential absorption of x-ray energy [1,14]. Tissue physical density is measured relative to the density of water and assigned a numerical value called a CT number or Hounsfield unit. The normal intervertebral disk is of uniform soft tissue opacity in CT images, with no visible distinction between the nucleus pulposus and annulus fibrosus [21]. The spinal cord, cerebrospinal fluid, and meninges are of similar tissue physical density and cannot be discriminated without the introduction of intra-thecal contrast media [8]. This combination of structures is referred to as the thecal sac in plain CT images. Epidural fat surrounds the thecal sac and is less dense than soft tissue, so it appears darker grey. This difference in tissue density allows discrimination of the outer margins of the thecal sac. Calcified disc material is visible in non-contrast enhanced CT images because it has a higher physical density than adjacent soft tissues and fat [25]. In CT images, extruded calcified disc material appears as a heterogenous mass that is more opaque (hyperattenuating) than the thecal sac. The degree of hyperattenuation increases with the degree of disc calcification. Chronic disc extrusions typically appear more smoothly-marginated, homogenous, and hyperattenuating than acute disc extrusions. Acute disc extrusions typically appear more ill-defined, and heterogenous. Acute disc extrusions are also more likely than chronic disc extrusions to be associated with a regional loss of epidural fat due to spinal cord swelling. Epidural hemorrhage may be seen as a rim of hyperattenuation that outlines the margins of the thecal sac cranial and caudal to the location of acutely extruded disc material.
For our study, medical records and digital CT images were retrieved and reviewed for 111 dogs with confirmed thoracolumbar disc extrusions in order to test the effects of MPR CT images on surgeon diagnostic performance. Surgeon diagnostic performance was assessed using questionnaires completed by three readers with prior experience performing surgeries in dogs with thoracolumbar disc extrusions. Effects were analyzed using diagnostic accuracy estimates, diagnostic certainty scores and interobserver agreement. We attempted to minimize learning curve effects by having readers interpret 2D images in a random order, then having readers interpret the MPR images in a re-randomized order. We found that diagnostic accuracy was significantly increased in one reader and diagnostic certainty was significantly increased in two readers for MPR versus 2D CT images. Our findings are consistent with those previously described in a study testing the effects of CT reformatting on surgical decision-making in humans with vertebral fractures [2].
The breed and sex distribution of our sample population was consistent with the populations described in two large outcome studies of dogs with disc extrusions [7,31]. The frequency of disc spaces affected was also representative. In our study, 75% of the lesions were in the T11-L2 region of the vertebral column. While most of the patients in our study were of chondrodystrophoid or small breeds, there was one German Shepherd Dog. This patient was included in the study because a disc extrusion was confirmed at surgery, and, while it is not common, large breed dogs have been reported to also suffer from this disease [6,22].
We used the surgical report as the gold standard for determining correct localizations of disc extrusions in our study. This gold standard was also used a recent report describing the diagnostic sensitivity of CT versus myelography for dogs with thoracolumbar disc extrusions [15]. However, previous studies have shown that surgical findings may not be the most reliable method for localization of IVDD [34]. Surgical visualization of extruded disc material may be limited by the size of the hemilaminectomy window, size of the thoracolumbar vertebral canal, and the amount of intra-operative hemorrhage. It is therefore possible that some of our readers' CT localizations were correct while the surgical report was not. However, we believe the fact that none of the patients used in this report required additional imaging studies or surgery during the same hospitalization period allows us to safely assume that all surgical procedures had been successful.
Reader diagnostic certainty for CT localizations was determined using a numerical scoring system of 1~10, with 10 indicating absolute certainty. Among the three readers, there was a 3~11% increase in mean diagnostic certainty scores for correct diagnoses using MPR CT images. Readers in our study were not timed for their evaluations of the image files, however most readers commented that more time was required to interpret 2D CT images versus MPR images. This time effect may have had an impact on diagnostic certainty scores for the 2D images. For future studies, perhaps a time restriction placed on the readers would increase the number of statistically significant differences in confidence or accuracy for 2D versus MPR images. Reader agreement was assessed using kappa statistics. We acknowledge that some researchers have questioned the interpretation of kappa statistics as raw numbers. However, the difference in agreement between 2D vs. MPR CT images increased for all our analyses (site, side, number affected) among all three readers. We therefore believe that the improved agreement identified in our study for MPR images is reliable.
Multi-planar reformatted views that our readers considered to be most helpful were the oblique transverse and curved dorsal MPR views. These views were most likely preferred because the location of disc material could be visualized relative to surgical landmarks such as the vertebral articular processes and the last pair of ribs. The last rib is the landmark used by most surgeons to determine the level of approach to the vertebral canal intra-operatively. Difficulty identifying this structure was commonly noted in readers' comments on the questionnaires. Oblique sagittal views were considered less helpful, most likely because it was difficult for readers to determine which side of midline was imaged. It was also difficult for readers to identify a landmark to use for identifying which vertebral locations were affected.
In conclusion, our findings indicate that MPR CT images can improve surgeon diagnostic performance for dogs with thoracolumbar intervertebral disc extrusions. Reformatting software is readily available to veterinarians, either through purchase or free download. While our study was restricted to thoracolumbar disc extrusions, it is likely that significant benefits could be gained from the application of this technology to other spinal diseases as well. Future research would be needed in order to confirm this.







 XML Download
XML Download