

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Diffusion-weighted imaging (DWI) visualizes the random microscopic mobility of water (Brownian motion) and thereby provides a tissue contrast that is different from that made with conventional T1-weighted (T1WI) and T2-weighted imaging (T2WI) [1-4]. DWI reflects changes in proton mobility caused by the alteration of tissue cellularity and the integrity of the cellular membrane, tortuosity of extracellular space, and viscosity of fluids due to pathologic processes [4-6]. Altering the gradient amplitude, duration, and time interval (b-value, measured in seconds per square millimeter) between paired diffusion gradients alters the sensitivity to the degree of water motion [7,8]. A higher b-value (b=e.g., 800 or 1,000 sec/mm2) has been recommended for the female pelvic region because it results in more diffusion weighting with better background suppression [1,4,8]. By performing DWI using different b-values, quantitative analysis, namely, the calculation of apparent diffusion coefficient (ADC) values, is possible and the ADC values can be displayed as a parametric map (ADC map) [8]. Restricted water diffusion demonstrates high signal intensity on DWI and lower ADC values on ADC map [1,7,8].
DWI was at first used in central nervous system imaging, especially in cases of acute ischemic stroke which causes a decrease of water diffusion compared with that of normal tissue [3]. DWI has been shown to be capable of detecting early or subtle changes within the brain before any visible abnormality appears on conventional imaging [8]. DWI has been prone to severe motion sensitivity due to the long scan times, because this will limit the effects of patient motion artifacts [9]. However, recent developments in fast magnetic resonance image (MRI) techniques have helped to overcome the difficulties, respiratory and bowel peristaltic motion, of abdominal and pelvic DWI and have increased the role and potential of MRI in evaluating the abdomen and pelvis [1]. Although performing DWI in the body is challenging because the inhomogeneity of the magnetic field over a large imaging area and susceptibility to motion artifacts related to respiratory and bowel peristaltic motion arising from different organs conspire to degrade image quality [9,10].
In general, malignant tumors have a higher cellularity than benign tumors; therefore, DWI can assist in differentiating malignant from benign tumors [11]. DWI is presently used for tumor detection, tumor characterization, and the evaluation of treatment response in patients with cancer [8]. Recent studies have described the usefulness of DWI for detecting malignant tumors of the liver, renal, prostate, colorectal, and pancreas [12-39]. Moreover, a quantitative analysis of ADC values can be used to characterize tumors and assess responses to treatment [40-45]. Other advantages of DWI include its cost-effectiveness and brevity of execution, its complete noninvasiveness, its lack of ionizing radiation, and the fact that no injection of contrast material is required [2,46-48].
In this article, we describe the clinical application of DWI in gynecological disorders and its diagnostic role therein. We used a DWI with a high b-value of 0 and 1,000 sec/mm2 and a reversed black-and-white gray scale.
DWI OF NORMAL FEMALE REPRODUCTIVE ORGANS
Normal structures, such as the premenopausal uterine endometrium and ovarian mesenchyme, excluding ovarian follicular cysts, show high signal intensity on DWI [49,50]. Interestingly, Kido et al. [51] observed cyclical changes in ADC values in the normal uterus during different menstrual phases in healthy reproductive age females. For the myometrium and endometrium, the mean ADC values tended to be lower in the menstrual phase than in other phases. The utility of DWI for detecting ectopically located abnormal gonads has been reported [4]. Normal or reactive lymph nodes and bowel mucosa are also hyperintense on DWI of the female pelvic cavity [7].
TUMOR DETECTION
On DWI, background tissues are relatively suppressed, whereas most forms of tumors show restricted water diffusion, which results in moderate to marked tumor conspicuity [1]. DWI may depict small-volume tumors which are not easily detectable by conventional imaging modalities [1]. Restricted water diffusion is generally considered associated with malignant tumors as a result of high cellularity [11]. Clinicians interpreting DWI in the abdominal and pelvic regions, however, should keep in mind that the likelihood that a lesion with restricted water diffusion is a benign disease was as high as 22% and that lesion with restricted water diffusion are much more likely to be malignant in patients with known malignant disease [52].
Namimoto et al. [47] showed a decision-making diagram in the MRI diagnosis of gynecological disorders with the addition of DWI and ADC values. ADC values may make it possible to differentiate between normal and cancerous tissues in the uterine cervix and endometrium, with cut-off ADC values of 1.4×10-3 mm2/sec and 1.15×10-3 mm2/sec, respectively. Among cystic ovarian lesions, most benign endometrial cysts and mature cystic teratomas had lower ADC values than malignant neoplasms, with cut-off ADC values of 2.0×10-3 mm2/sec. Detection oh high signal intensity on DWI may be useful for evaluation of peritoneal dissemination.
The ADC values may vary on acquisition parameters associated with b-values, magnetic field strength (3.0 T vs. 1.5 T), and breath-holding technique [53]. Thus absolute quantification is hampered by the fact that ADC values are influenced by all of these technical factors.
Due to the relatively poor spatial resolution of DWI, it is difficult to define the anatomic location of the abnormal signal on DWI, especially in small lesions, such as peritoneal implants or small recurrence or lymph node metastasis. One can resolve this problem by using recently developed fusion software that can automatically overlay the DWI onto conventional MRI. Even without the fusion software, one can correlate the location of signal on the DWI with conventional MRI [4].
1. Gynecological malignant tumors
Cervical cancer has demonstrated significantly lower ADC values than normal cervical tissues [1,6,46,47,54]. Moreover, according to Liu et al. [55], squamous cell carcinoma of the uterine cervix tends to demonstrate lower ADC values than adenocarcinoma, providing a means to predict the histologic type of uterine cervical cancer to some extent. Similar findings to cervical cancers have been noted in endometrial cancers (Fig. 1), with a tendency toward lower ADC values in highergrade lesions [1,3,6,47,49].
2. Peritoneal dissemination
The peritoneal cavity is a common site of metastatic spread for gynecological malignant tumors, especially ovarian cancer [2,56-58]. On DWI, ascites and most bowel contents have suppressed signal intensity, while peritoneal dissemination involving the bowel shows high signal intensity [57]. Thus increasing the conspicuity of the dissemination site, DWI has a high accuracy at detecting peritoneal dissemination [56,57]. Sensitivity and specificity of depicting peritoneal dissemination with the combination of DWI and conventional MRI, DWI alone, and conventional MRI alone were reported as 84% and 91%, 71% and 90%, 52% and 92%, respectively [56].
3. Recurrent disease
As with the case of peritoneal dissemination, DWI may be also useful in depicting small recurrent disease, such as in the vaginal cuff site (Fig. 2). Small recurrent disease, covered by the serosal surface of intestinal loops and solid viscera are difficult to detect with computed tomography (CT) or conventional MRI, because they are masked by the similarity of their attenuation or signal intensity to that of adjacent structures [50].
4. Lymph node staging
Evaluation of pelvic lymph node status is important in devising a treatment plan in gynecologic malignant tumors. The differentiation between benign and malignant nodes in the pelvic cavity remains challenging for imaging, because the morphological criteria including size, shape or presence of necrosis, has so far not been absolutely reliable with enlarged reactive lymph nodes and malignant non-enlarged lymph nodes [59-62].
Diagnoses of lymph node pathology by conventional MRI and CT are based on roughly defined size and morphologic criteria. The sensitivities for conventional MRI or CT in detecting lymph node metastases in gynecologic malignant tumors range from 43% to 73% [63,64]. Some reports have demonstrated the usefulness of DWI and ADC values in the detection of metastatic lymph nodes in gynecological malignant tumors [61,65,66].
Lin et al. [65] evaluated for detection of pelvic lymph node metastasis in patients with cervical and endometrial cancers on DWI. The combination of size and relative ADC values was useful compared with conventional MRI in detecting pelvic lymph node metastasis in patients with cervical and endometrial cancers, and the sensitivity and specificity were 83 and 25% with cervical cancer, 99 and 98% with endometrial cancer, respectively [65]. Kim et al. [61] reported the ADC values were significantly lower in the metastatic lymph nodes than in the nonmetastatic lymph nodes of cervical cancer patients, and the area-under-the-curve of ADC values for differentiating metastatic from nonmetastatic lymph nodes was 0.902×10-3 mm2/sec. With this threshold, the sensitivity and specificity of ADC values for differentiating metastatic from nonmetastatic lymph nodes were 87% and 80%, respectively. Measurement of ADC values may be useful, especially for detection of small metastatic lymph nodes compared with the limited sensitivity of CT and conventional MRI [59,61]. DWI shows relatively poor anatomical detail, fusion of DWI with T2WI improves identification of pelvic lymph nodes and their metastases [7,59,60,67]. On the contrary, some reports showed that the role of DWI and ADC values in distinguishing benign and malignant lymph nodes is limited [7,50,59,68], because cellular tissues such as lymph nodes have high signal intensity on DWI regardless of their biologic behavior [60,69]. There is still considerable overlap, however, in ADC values, and lymph node evaluation in clinical practice has to continue to rely on conventional features such as shape, size, and growth patterns [52].
LESION CHARACTERIZATION
Differences in tumor cellularity may reflect their histologic composition and biologic aggressiveness [8]. Additional information obtained from a quantitative analysis of ADC values can be used to characterize tumors [6]. However, there are some difficulties due to the considerable overlap in ADC values of benign and malignant tumors [8]. Even in malignant tumor necrosis, edema or cystic components show increased water diffusion due to the decrease in tumor cellularity. Therefore, interpretation of DWI requires consideration of the patient's clinical presentation and history, as well as a morphological assessment by conventional MRI [1].
1. Uterine myometrial lesion
As pathological evaluation of uterine myometrial lesions is difficult, imaging diagnosis is important. However, since uterine sarcomas are occasionally associated with various types of degeneration or cellular histologic subtypes, strict differentiation of benign and malignant myometrial tumors on the basis of MRI findings may be difficult [47,70]. Tamai et al. [71] reported that DWI may be an additional tool for distinguishing uterine sarcomas from benign leiomyomas (Fig. 3); however, the ADC values overlap with those of ordinary leiomyomas and cellular leiomyomas.
2. Tumors in the uterine endometrial cavity
ADC values provide useful information in differentiating malignant (endometrial carcinoma and carcinosarcoma) from benign (submucosal leiomyoma and endometrial polyp) endometrial cavity lesions [71].
3. Adnexal lesions
An ovarian mass with a solid component was classically predictive of a malignant tumor [72]. However, many benign ovarian masses can display a solid component including fibromas, cystadenofibromas, Brenner tumors, sclerosing stromal tumors, and theca cell tumors. The addition of DWI improved the MR characterization of complex adnexal masses compared with conventional MRI alone; indeed, DWI has recently been shown to be effective in the differentiation of benign from malignant adnexal masses [73,74]. Therefore, a solid component in an adnexal mass with a high signal intensity on DWI is predictive of malignant tumors (Fig. 4) [4,74,75]. According to Takeuchi et al. [75], the mean ADC values between the benign and malignant ovarian tumors differed significantly. Using a cutoff ADC value of 1.15 ×10-3 mm2/sec, differentiating benign from malignant/borderline malignant lesions had a sensitivity of 74%, specificity of 80%, positive predictive value (PPV) of 94%, and negative predictive value (NPV) of 44%. Using a cutoff ADC value of 1.0 ×10-3 mm2/sec, differentiating benign from malignant/borderline malignant lesions had a sensitivity of 46%, specificity of 100%, PPV of 100%, and NPV of 32%. However, there were some overlaps between the mean ADC values of the malignant and benign ovarian lesions. They considered that their results may reflect the increased mean ADC values in some malignant lesions owing to the existence of small necrotic or cystic areas in solid tumoral components, or fluid collection intervening papillary projections, and the decreased mean ADC values in some benign lesions owing to relative hypercellularity in functioning ovarian tumors such as thecomas, or restriction of the water diffusion by dense stromal proliferation in fibroma without edematous changes [75]. In addition, a study by Thomassin-Naggara et al. [74] showed that a solid component that exhibits low signal intensity on both T2WI and DWI was always benign (Fig. 5). Some reports showed that ADC values may provide limited information in the differential diagnosis of a cystic ovarian tumor [76,77]. Due to the morphological and histological variety of ovarian tumors, DWI may have a role in the preoperative evaluation of ovarian tumors. This is also useful to determine operative strategy, including the planning of the operation method, expectant management, or possibility and the feasibility of laparoscopy and conservative surgery [74]. However, according to Namimoto et al. [47], ADC values varied widely among malignant ovarian tumors, a phenomenon attributable to their morphological and histological variety.
MONITORING TREATMENT RESPONSE
DWI shows promise as a biomarker for tumor treatment responses [1,2,7,47,78-80]. Increases in ADC values would reflect an increase in the mobility of water, either through the loss of membrane integrity or a change in the relative volume of extracellular space with a corresponding decrease in cellular size or number, as seen with necrosis or apoptosis due to tumor treatment (Fig. 6) [78,81]. In short, this approach is based on early cellular changes in the tumor on initiation of effective chemotherapy or radiation therapy [52]. Furthermore, treatment effects can be observed within the first 24 hours after initiating treatment due to cell swelling, which results in a transient decrease in ADC values [8]. In tumor treatment, the change in ADC values accurately reflected a change in cellularity and could be measured earlier than changes in tumor volume, and ADC values have been used to characterize tumors and quantify treatment-induced changes, which may occur earlier than conventional morphologic alterations [78,80,82-86]. A recent study evaluated ADC histograms in the prediction of chemotherapy response in patients with metastatic ovarian or primary peritoneal cancer [80]. The study indicated that an early increase of ADC values and later decrease of histogram skew and kurtosis can detect chemotherapy response assessed with integrated morphologic (size reduction) and biochemical (serum CA-125 level) criteria. Several studies have shown that cellular tumors with low baseline pretreatment ADC values responded better to chemotherapy or radiation treatment than tumors with high pretreatment ADC values [87-89]. One possible explanation is that necrotic tumors, which exhibit higher ADC values, are frequently hypoxic, acidotic, and poorly perfused, leading to diminished sensitivity to chemotherapy and radiation therapy [8].
WHOLE-BODY DWI
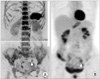
Whole-body DWI was first reported in 2004 by Takahara et al. [69], and constituted a unique concept, called "diffusion-weighted whole-body imaging with background body signal suppression" (DWIBS) [90]. Potential clinical applications of whole-body DWI include cancer staging because both the primary tumor and distant metastases demonstrate restricted water diffusion [1,90]. Accordingly, whole-body DWI has the potential for use in tumor staging, detecting responses to cancer therapy, and detecting tumor persistence or recurrence [90]. Three-dimensional (3D) display of DWI with a reversed black-and-white gray scale can produce positron emission tomography (PET)-like images (Fig. 7) [4,91].
Komori et al. [92] reported that a larger number of malignant tumors were detected visually with whole-body DWI than with PET/CT. However, according to Satoh et al. [93], PET/CT proved to be more reliable than DWI and contrast-enhanced CT (CE-CT) in the detection of peritoneal dissemination. The sensitivity of PET/CT, DWI, and CE-CT were 94%, 85%, and 83% and the specificity were 94%, 89%, and 87%, respectively [93]. Nevertheless, DWI may still be of value because it showed satisfactory sensitivity for lesions and can be used as a screening tool because of its excellent lesion specificity [93]. The advantages of DWI compared with PET/CT include its noninvasiveness and relatively low cost [93]. However, whole-body DWI does have several limitations [90]. First, whole-body DWI does not exclusively visualize malignant tumors, as benign pathologies with restricted water diffusion such as abscesses also exhibit high signal intensity on whole-body DWI [90]. Second, whole-body DWI also visualizes numerous normal structures; namely, the brain, salivary glands, tonsils, spleen, gallbladder, small intestine/small intestinal contents, colon, adrenal glands, prostate, testes, penis, spinal cord, peripheral nerves, lymph nodes, bone marrow, endometrium and ovaries may all exhibit high signal intensity [90]. Another limitation is the lack of sufficient anatomical information [90]. According to Low [1], whole-body DWI seems unlikely to entirely replace PET/CT, because whole-body DWI does not provide true metabolic information. Low [1] advocated that initial evaluation with PET/CT might be used to identify sites of primary and metastatic tumor, and follow-up whole-body DWI could be performed to monitor the tumor response to therapy.
PITFALLS
1. T2 shine-through effect
One of the pitfalls of visual assessment of DWI is known as the T2 shine-through effect [8]. Because the signal intensity on DWI can be influenced by the signal intensity on T2WI, high signal intensity tissues on T2WI may exhibit increased signal intensity on DWI [47]. ADC map eliminates the effect of T2 decay. In cases of high signal intensity on DWI, evaluation of T2WI as well as an ADC map, which depicts changes in signal intensity that are solely caused by diffusion, are required [1].
3. Ovarian cystic lesions with water diffusion restriction
DWI is useful for tumor characterization, namely differentiating malignant and benign lesions. However, abscesses, mature cystic teratomas, and hemorrhagic cysts such as endometriotic cysts may show high signal intensity on DWI and lower ADC values than other benign ovarian cysts [47,94-96]. Water diffusion in abscesses is restricted due to the paramagnetic properties of cystic components. In the majority of mature cystic teratomas, conventional MRI with fat saturation may be sufficient for making a correct diagnosis [76]. According to Nakayama et al. [76], mature cystic teratomas are lined with a keratinized squamous epithelium in most cases; by contrast, fatty components and calcification are pathologically found in 67-75%. Keratinoid substances restrict water diffusion in mature cystic teratomas [76]. DWI and ADC values may be useful and serve as an adjunctive tool to ensure the accuracy of the diagnosis, particularly in patients with a teratoma with paucity of fat (Fig. 8) [76]. Endometriotic cysts tend to contain hemoglobin degeneration products, and its viscosity lowers ADC values [47]. On the contrary, detection of a malignant lesion, such as malignant transformation of a mature cystic teratoma or a malignant tumor arising in an endometriotic cyst, might be difficult, because the entire cystic component may show high signal intensity on DWI.
4. Inflammatory lesion
A solid adnexal mass with high signal intensity on DWI within a solid component is predictive of malignancy, as mentioned above. Inflammatory, granulomatous adnexal lesions may show morphologically solid and restricted water diffusion on MRI and can mimic a malignant tumor (Fig. 9). Oussalah et al. [97] reported restricted water diffusion in the inflamed bowel of a Crohn's disease patient; this restricted water diffusion in active Crohn's disease is explained by the strong association with lymphoid aggregates.
CONTROVERSY
In gynecologic disorders, conventional morphologic evaluation on T1WI and T2WI is essential. DWI should be utilized as a complementary sequence to conventional morphologic imaging. Because DWI has relatively poor spatial resolution, detection of small lesions on DWI may be limited. It is necessary to refer to other imaging sequences or fusion images for sufficient identification of lesion boundaries [47]. Moreover, a major challenge to the widespread implementation of DWI is the lack of an acceptable standard approach to data collection and analysis [8,56]. Standardization will allow for improved repeatability and reproducibility based on diffusion indices [2]. Reproducible measurements are particularly important to determine both the limits of using quantitative ADC values to discern the magnitude of change and whether DWI measurements are to be routinely used for monitoring therapeutic effects [8].
CONCLUSION
Functional imaging is becoming increasingly important in the evaluation of cancer patients because of the limitations of morphologic imaging [1]. DWI can be applied widely for tumor detection and tumor characterization and for the monitoring of response to treatment [47]. However, since there are some overlaps on DWI between benign and malignant gynecological disease, DWI evaluation of the lesion should be done in concert with conventional imaging, to distinguish between benign and malignant gynecological disorders [47]. The advantages of DWI include its cost-effectiveness and brevity of execution, its complete noninvasiveness, its lack of ionizing radiation, and the fact that it does not require injection of contrast material, thus enabling its use in patients with reduced renal function [2,8,47,48]. DWI could provide supplemental information in patients with gynecological disorders and could easily be incorporated into standard clinical protocols utilizing MRI [47,78,90].








 XML Download
XML Download