

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Various innovative surgical techniques have been proposed to improve the outcomes of adult living donor liver transplantation (LDLT) because vascular complications occurred in a not negligible proportion of LDLT recipients. On comparing with deceased donor liver transplantation, the most noticeable technical difference in LDLT is hepatic vein reconstruction. The hepatic venous drainage pathways of a right liver graft consist of the right hepatic vein (RHV), the middle hepatic vein (MHV) and the inferior RHV. Complete reconstruction of these venous outflow pathways is essential to prevent detrimental hepatic venous congestion. To match the graft hepatic veins to the recipient inferior vena cava optimally, various innovative surgical techniques have also been developed because there are numerous anatomical variations in the donor and recipient hepatic veins.12345
Individualized reconstruction techniques customized to each LDLT operation have contributed to a decrease in vascular complications, but it is technically complex and demanding to achieve optimal individualization. We have shown that implantation of a standardized right liver graft would be more effective in minimizing vascular complications than customized individualization.6 Thus, we intended to present the details of surgical techniques for right liver graft standardization and its implantation.
Go to : 
STANDARDIZATION OF A MODIFIED RIGHT LIVER GRAFT (VIDEO PRESENTATION)
Right liver graft standardization intends to provide hemodynamics-based and regeneration-compliant reconstruction of vascular inflow and outflow. Right liver graft standardization consists of the following components: RHV reconstruction includes a combination of caudal-side deep incision and patch venoplasty of the graft RHV to remove the acute angle between the RHV and the inferior vena cava (Fig. 1);5 MHV reconstruction includes interposition of a uniform-shaped conduit with large-sized homologous or prosthetic grafts (Fig. 2);2789 If the inferior RHV is present, its reconstruction includes funneling and unification venoplasty for multiple short hepatic veins (Fig. 3);10 If donor portal vein anomaly is present, its reconstruction includes conjoined unification venoplasty for two or more portal vein orifices (Fig. 4).1112
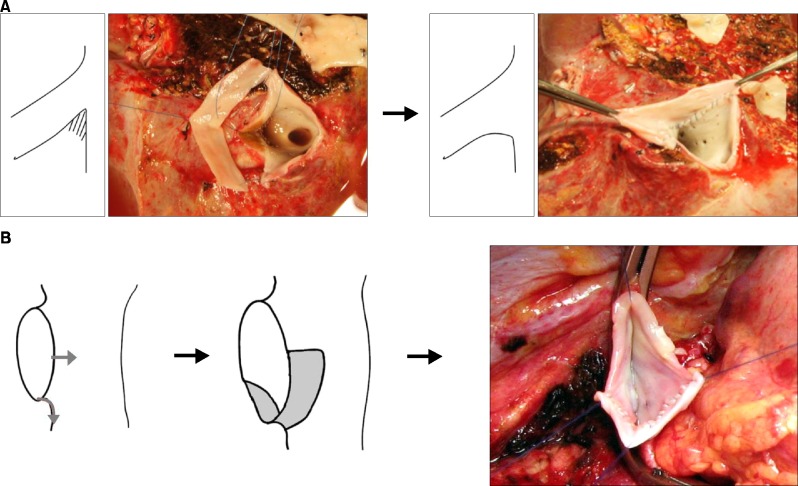 | Fig. 1Right hepatic vein (RHV) reconstruction technique with RHV angle blunting and inferior vena cava enlargement. The central defect was firmly tied for bleeding control and patch coverage and then the suture was extended bidirectionally. (A) After caudal incision of the RHV orifice, a vein patch was attached to the defect. (B) Recipient RHV stump was incised by sequential longitudinal and transverse incisions, and then a small vein patch was attached to the inferior vena cava.5
|
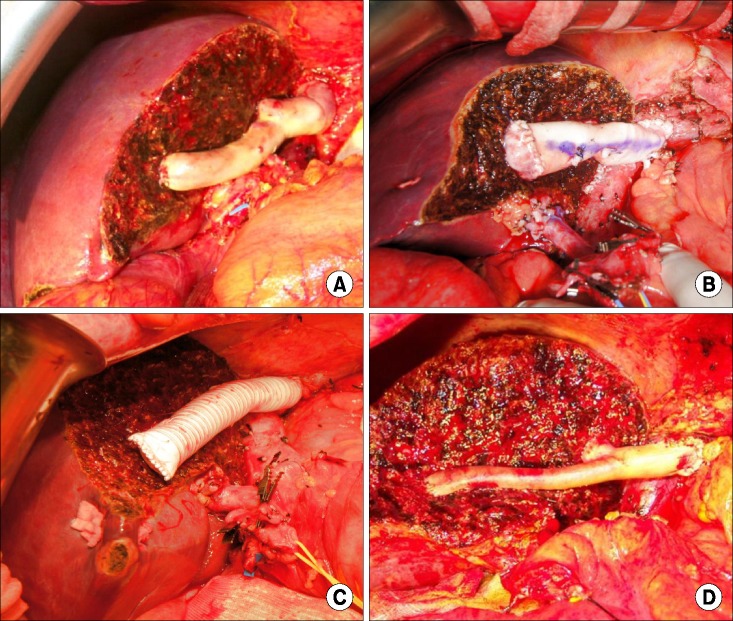 | Fig. 2Middle hepatic vein reconstruction using a cryopreserved iliac vein graft (A), a cryopreserved aorta graft (B), a polytetrafluoroethylene grafts, (C) and a cryopreserved iliac artery graft (D).789
|
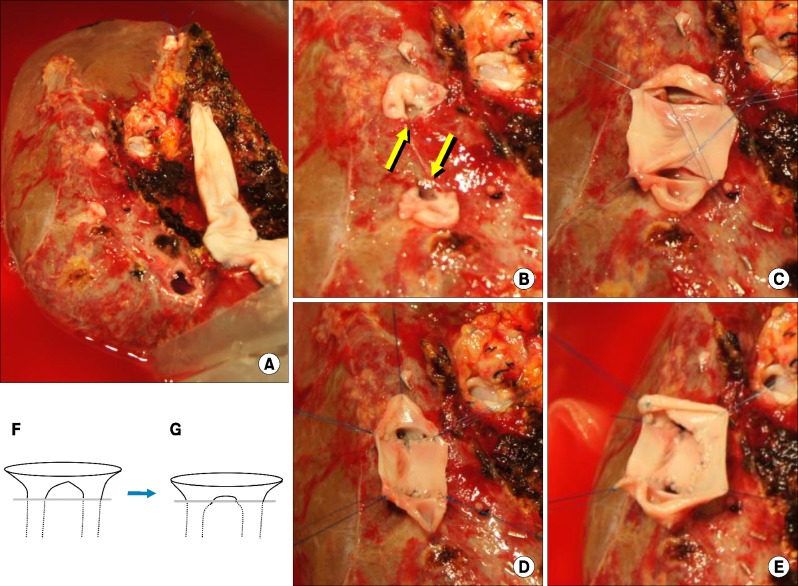 | Fig. 3Refined surgical techniques for reconstruction of two adjacent small-sized inferior right hepatic veins. A narrow vein neck (A) was opened by a small incision (arrows) into the liver parenchyma (B). A small vein patch was tightly placed between the incised orifices (C) and then sutured (D). Two thirds of the orifice circumference was fenced with a narrow vein patch to facilitate reconstruction at the recipient inferior vena cava (E). Additional small incisions converted a conventional unification venoplasty (F) to a unification funneling venoplasty (G), making it hemodynamically more resistant to stretching or compression.10
|
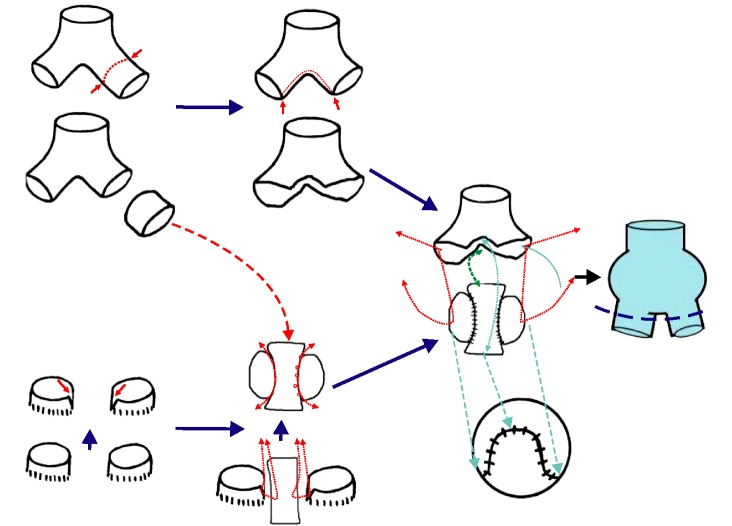 | Fig. 4Schematic illustration of the conjoined unification venoplasty technique. A 5 mm-long segment of the autologous sectional portal vein (PV) branch was excised and inserted as a central vein patch between the two sectional PV orifices with small niches. The crotch-opened autologous Y-graft was anastomosed to the unified graft PV orifice, making a potbelly-shaped PV confluence.11
|
This 8 minute-long video clip that shows the surgical technique from bench to reperfusion was presented at the 22nd Annual International Congress of International Liver Transplantation Society (ILTS) held in Seoul, Korea.
The recipient was a 54-year-old male patient with hepatitis B virus-associated liver cirrhosis. The living donor was his 23-year-old son. A right liver graft with complete preservation of the donor MHV was harvested. The graft weight was 643 g, which was equivalent to 1.03 of the graft-recipient weight ratio. The graft had two segment V vein (V5) branches and one segment VIII vein (V8) branch. The two V5s were first unified with a small patch of cryopreserved iliac vein. A long cryopreserved iliac vein conduit was used to reconstruct the MHV trunk with grafts V5 and V8. Caudal-side deep incision and venoplasty using an autologous greater saphenous vein patch were performed for the graft RHV. In the recipient, caudal extension venoplasty with an autologous greater saphenous vein patch was performed for the RHV. A large anastomosis with a 3.5 cm-long cephalocaudal diameter was performed for RHV reconstruction. The recipient portal vein was transected close to the hepatic parenchyma in order to use the portal bifurcation as a branch patch. A panning suture technique was used to adjust the size discrepancy between the graft and recipient portal vein orifices. The MHV conduit was anastomosed with the recipient MHV-left hepatic vein trunk stump in an end-to-end fashion. After portal reperfusion, there was only a scanty amount of hepatic venous congestion in the right liver graft. Right hepatic artery reconstruction under surgical microscopy was followed by duct-to-duct biliary reconstruction. Both the donor and the recipient recovered uneventfully after surgery. The recipient is doing well without any vascular complication for 1 year after LDLT.
Go to :
DISCUSSION
The patient survival outcome after customized individualization of vascular reconstruction was excellent, but we observed that a small proportion of patients are still at risk of vascular complications due to unusual liver anatomy and/or inappropriate reconstruction customization. After having experienced more than 2000 cases of adult LDLT,113 we established the concepts of right liver graft standardization, in which every component of vascular reconstruction was repeatedly verified to observe whether the principles of hemodynamics are followed and whether it would be fully compliant with graft regeneration.6
In adult LDLT using a modified right liver graft, in order to maximize donor safety through donor vessel-sparing, the inferior RHV should have only one unified orifice; the MHV trunk should not be harvested; and the main trunk of the anomalous donor portal vein should be fully preserved. Both individual customization and general standardization methods make the graft inflow and outflow vascular orifices suitable for reconstruction through time-consuming back table work. Once a uniform type of standardized right liver graft is created, it helps in making the recipient-side operation simple and straightforward, resulting in a decrease in vascular complications. The beneficial effects of right liver graft standardization may finally lead to a decrease in overall donor and recipient complication rates.6
Our intention behind proposing the concept of right liver graft standardization is that it can be universally applicable and may guarantee nearly the same outcomes regardless of the surgeon's experience. We believe that this reconstruction model would be primarily applied to a majority of adult LDLT cases; thus, only a small proportion of LDLT cases may require individualized case-by-case modification due to major donor anomalies or unusual anatomical distortion in the recipient.
Go to :

 XML Download
XML Download