

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Anomalous portal vein (PV) branching of the right liver is encountered in a considerable proportion of normal individuals.1 Presence of graft double PV orifices requires unification procedures at the bench. Autologous portal Y-graft (PYG) interposition has long been accepted as the standard procedure due to acceptably low rates of early PV stenosis with excellent long-term patency rates.2345 However, in our experience, the surgical technique for PYG interposition was often demanding due to its low tolerance to PV alignment error.6 We introduced the surgical technique of conjoined unification venoplasty (CUV) as a refined alternative to conventional autologous PYG interposition. This newly developed technique has been accepted in our institution as one of the preferred technical options for double PV reconstruction.78
In this case report, we presented the clinical application of CUV to the triple PV openings of a right liver graft and discussed technical aspects for further application.
Go to : 
CASE PRESENTATION
The recipient was a 32-year-old male patient with hepatitis B virus-associated liver cirrhosis. The living liver donor was his 33-year-old sister. The recipient was ABO blood group-incompatible, thus preparation with rituximab and plasma exchange therapy was performed according to the institutional protocols.9
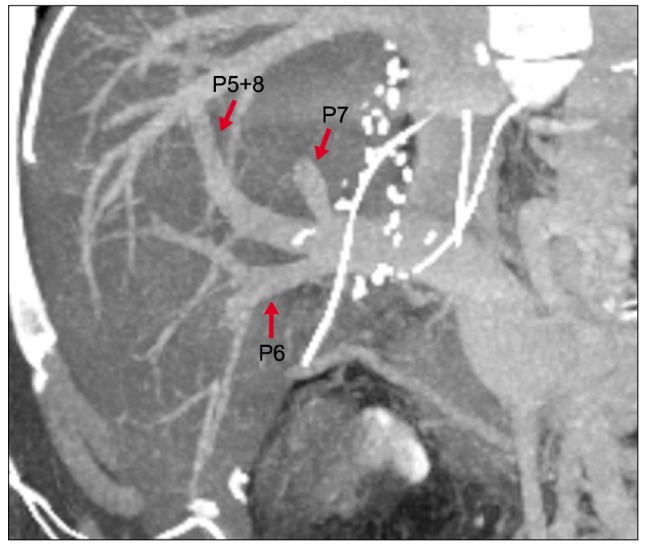
The donor liver has a type III PV anomaly, but the right posterior PV branch was bifurcated early into separate branches of the segments VI and VII (Fig. 1). To ensure prevention of iatrogenic injury to the donor's remnant PV, three right liver PV branches (one branch to the right anterior section and one each to the segment VI and VII) were cut separately (Fig. 2A).
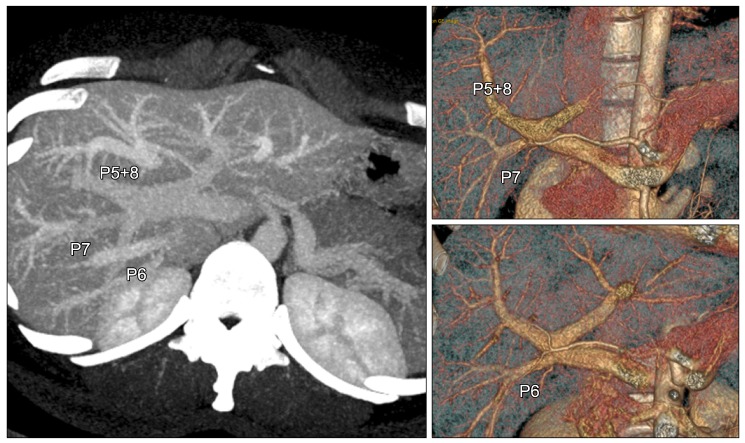 | Fig. 1Computed tomography portogram images showing triple branching of the right portal vein. P5+8 indicates the right anterior section (segments V and VIII) branch; P6 and P7 indicate the branches to the segments VI and VII.
|
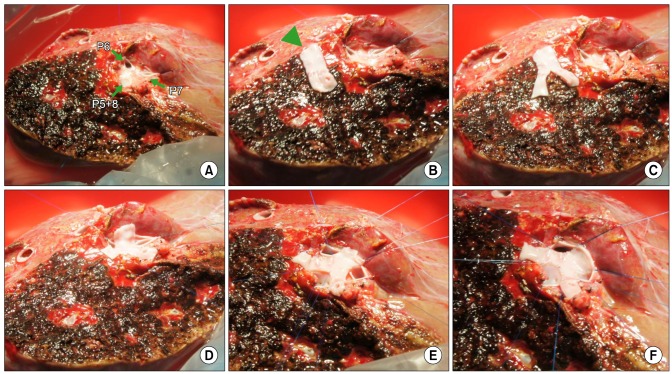 | Fig. 2Operative photographs to unify the portal vein (PV) branches. Three PV orifices (A) were unified using a Y-shaped central patch of recipient's greater saphenous vein (B-F). A small niche was made at each PV orifice to elongate the suture lines (E). Arrows indicate PV orifices. An arrow head indicates the greater saphenous vein patch.
|
The CUV technique was selected for secure reconstruction of these three PV branches.8 This technique consists of placement of a small vein unification patch between three PV orifices, followed by overlying coverage with a crotch-opened autologous PYG. To unify these three PV orifices as simply as possible, a short segment of autologous greater saphenous vein (GSV) patch was used. A short longitudinal incision was applied to this GSV patch in order to compensate the central defect among the three PV orifices. The Y-shaped GSV patch was attached to conjoin the three PV orifices by using bidirectional running sutures; and, a small niche was made at each PV orifice to elongate the suture lines, which would act as a source for growth factors. In addition, each end of GSV patch was made redundant, which would act as another source for growth factor (Fig. 2B-F).
At this time, the recipient's autologous PYG was excised. The crotches of the right anterior and posterior sectoral PV branches and left first-order PV branch were incised to make a wide orifice. The wide V-shaped wall defects between the right anterior sectoral and left PV branch walls were sutured to facilitate anastomosis to the graft PV orifice. Bidirectional running sutures were made at each PV orifice after fixation suture at the inner most side of each PV orifice. Three bidirectional running sutures were placed for complete attachment of the crotch-opened autologous PYG. The internal suture lines were mechanically dilated with blunt tonsil forceps (Fig. 3A-E).
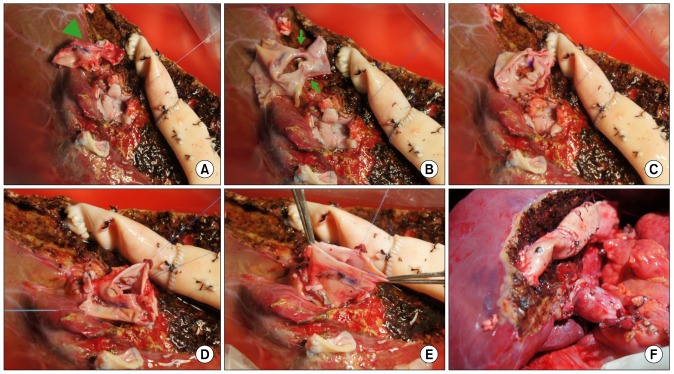 | Fig. 3Operative photographs to attach the recipient portal vein (PV) graft. Recipient's autologous portal Y-graft (arrow head) was excised (A). PV crotches were incised to make a wide common orifice and the V-shaped wall defects (arrows) were sutured (B, C). This PV patch was attached with three bidirectional running sutures (D, E). The graft PV was anastomosed with the recipient PV stump (F).
|
The graft weight was 760 g, which was equivalent to 1.24 of graft-recipient weight ratio. This graft PV was anastomosed with the recipient's remnant PV stump. After portal reperfusion, the conjoined PV portion bulged like a tennis ball, thus providing a wide tolerance toward alignment mismatching of PV anastomosis (Fig. 3F).
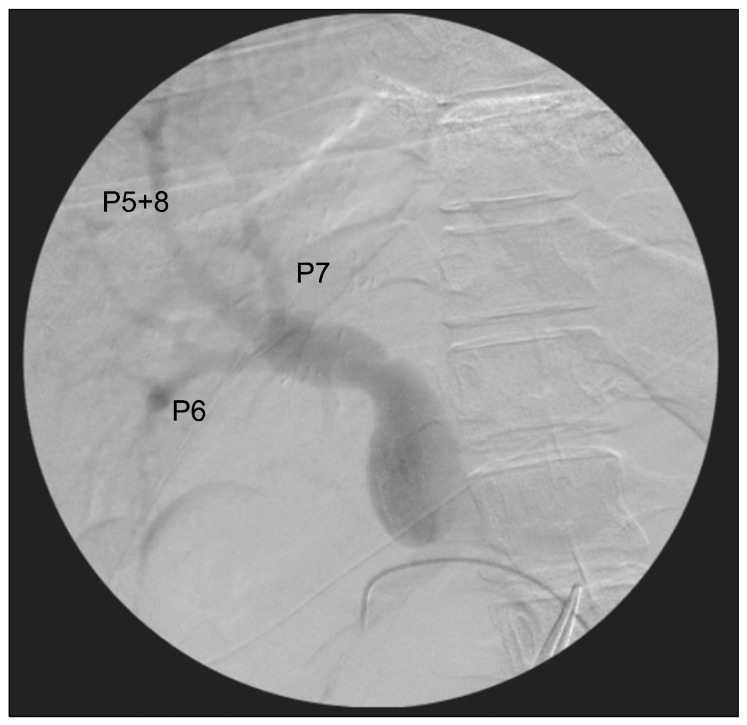
For occlusion of the portal collateral veins, an intraoperative direct portogram indicated that the shape of the conjoined three PV branches was nearly the same as that in the donor portal anatomy (Fig. 4). Computed tomography images at 1 week post-liver transplantation showed that the recipient PV anastomosis appeared naturally streamlined (Fig. 5), which was quite similar to the original preoperative shape of donor PV confluence. The patient recovered uneventfully from the living-donor liver transplantation operation.
Go to :
DISCUSSION
Following its first introduction in 2014, CUV has been rapidly accepted as one of the standardized procedures for multiple graft PV orifices of right liver graft in our institution.8 Conventional PYG interposition appears to be intuitively simple and theoretically ideal, but in practice, it was often technically demanding, primarily due to anatomical variations and discrepancies between the recipient and graft PVs. Direct PYG interposition is not applicable to the graft triple PV orifices, as in the present case.
The surgical technique for CUV appears to be very flexible and tolerant, thus it is readily modifiable with minor technical refinements. The technical refinements applied to this case were as follows: a central GSV patch was incised to make a Y-shape to match the central defect; the end portions of GSV patch were left as redundant and small niches were applied to elongate the suture lines; V-shaped defects at the crotch-opened autologous PYG patch were repaired to facilitate continuous sutures; and mechanical dilatation was applied to the internal suture lines. The CUV procedure is still evolving technically due to necessity from anatomical variations of the donor PV. The most important technical point is to make the PV confluence portion large enough, such that most anatomical variations and discrepancies between the recipient and graft PVs are spontaneously resolved following the principles of fluid dynamics.78
Intraoperative portogram and 1-week computed tomography images with 3-dimensional reconstruction indicated that the intraluminal images of conjoined-and-unified PV reconstruction were very similar to those of single PV reconstruction. This was suggestive of excessive expansion of the PV confluence portion at the time of portal reperfusion, but rapid reshaping develops following the principles of hemodynamics. Our CUV technique that ensures secure PV reconstruction is one of the essential components of graft standardization for living-donor liver transplantation.1011
We have previously reported8 that the primary indications of CUV include a combination of one small and one large sectional PV orifices, presence of a small accessory third PV branch, long extrahepatic PV branch, widely separated PV orifices, and poor conditions of autologous PYG, and multiple sizable PV orifices. As its indications are wide, it must contribute to ensuring the safety of living donors, because excessive excision of the donor PV is unnecessary. Donor surgeons should be aware that excessive resection of donor PV is highly associated with donor PV stenosis.412
In conclusion, the CUV technique enabled uneventful reconstruction of triple donor PV orifices. Thus, CUV can be a useful and effective technical option for reconstruction of right liver grafts with various anomalous PVs during LDLT.
Go to :
 XML Download
XML Download