

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cholelithiasis is one of the most common conditions that requires surgical intervention in Europe and the United States. According to the literature, roughly 10-15% of the population may suffer from cholelithiasis, and 3-10% of patients who undergo cholecystectomy may have stones in the common bile duct (CBD).1
Laparoscopic cholecystectomy is one of the most frequently performed surgical interventions; however, intraoperative control of the patency of the CBD is not performed routinely in patients who are in the low risk category for probable choledocholithiasis. Simple laparoscopic cholecystectomy is recommended if magnetic resonance cholangiopancreatography (MRCP) confirms the absence of biliary stones in the CBD, or the patient has undergone endoscopic preoperative clearance of the CBD.
Endoscopic retrograde cholangiopancreatography (ERCP) typically combined with sphincterotomy, is a routine therapeutic procedure for cases with confirmed stones in the CBD. However, it is associated with a relatively high complication rate, including post-ERCP pancreatitis, and is therefore less useful in patients with biliary pancreatitis.23 Technical skill and proper clinical indications for the procedure is a major determinant for success, rather than the age or the general medical condition of the patient.2 Laparoscopic treatment of emergent patients with a complicated gallstone disease is more challenging due to the limited time for preoperative MRCP or ERCP. Surgical intervention is often more complicated due to edema and inflammation. Although intraoperative cholangiography may improve the diagnostic accuracy, it is associated with a 5.1% unsuccessful procedure rate, increased operative time and a 15-20% rate of overlooked biliary stones.456 Laparoscopic intraoperative ultrasonoscopy (US) is an essential and reasonable alternative to intraoperative cholangiography and, in combination with laparoscopic choledochoscopy, increases the options of exploring the CBD during the surgical intervention.
The aim of our study was to assess postoperative course of cholangitis and biliary sepsis after laparoscopic clearance of the CBD in emergently admitted patients with choledocholithiasis and cholangitis.
Go to : 
MATERIALS AND METHODS
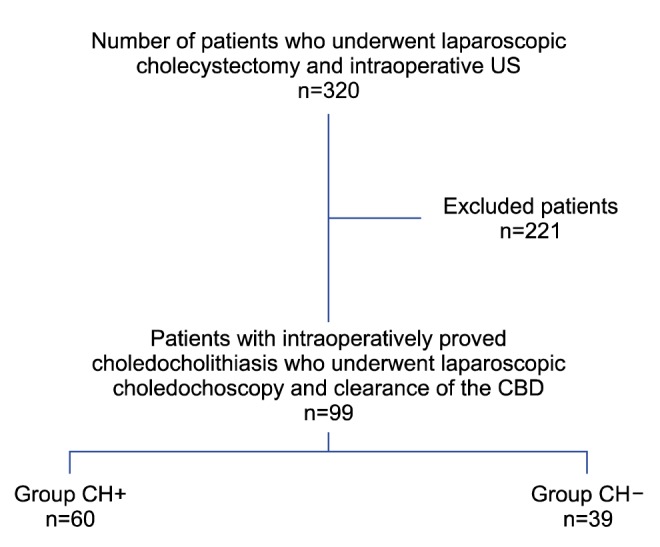
Patients with symptomatic gallstone disease and suspected choledocholithiasis who were urgently admitted to the hospital and eligible for laparoscopic clearance of the common bile duct, were prospectively included in the study during the period from August 2012 to December 2014 (Fig. 1). Patients were stratified in 2 groups according to the preoperative presence or absence of cholangitis for assessment of the postoperative inflammatory response. Suspicion of choledocholithiasis was based on evidence of cholangitis, biliary pancreatitis and/or characteristic symptoms complex of Charcot's triad frequently accompanied by pale stools and dark urine.
Preoperative diagnosis of cholangitis was based on criteria recommended in the Tokyo Guidelines 2013, i.e., evidence of inflammatory response (increased leukocytes >10×1000/µl) or C-reactive protein more than 10 mg/L, cholestatic pattern presented by abnormal liver function tests (alkaline phosphatase, gamma-glutamyl transferase, aspartate aminotransferase, and alanine aminotransferase ≥1.5 of upper normal limit) or total bilirubin ≥34.2 µmol/L and gallstones in the gallbladder and/or dilatation of the common bile duct >6 mm confirmed by transabdominal US.67 The diagnosis of biliary pancreatitis was made when 2 of the following revised Atlanta 2012 criteria were presented - abdominal pain consistent with acute pancreatitis; serum lipase activity >3 over the upper limit of normal; and characteristic findings of acute pancreatitis on radiological investigations.8 Preoperative anesthesiological status was assessed in all patients using the American Society of Anaesthesiologists Physical Status classification system (ASA score).910
Patients were stratified in 2 groups according to the presence of acute cholangitis (CH+ group) or the absence of cholangitis (CH- group). Laparoscopic intervention was performed using the standard 4-troacar technique and started with the dissection of Callot's triangle. The cystic duct and artery were clipped and the cystic artery was divided. The gallbladder was left in situ and retracted during the intraoperative US investigation, performed with BK Medical flex Focus 800 US machines and special flexible laparoscopic transducer 8666-RF. All examinations were performed by 2 specially trained surgeons. The US probe was inserted through the epigastric trocar and placed on the superior edge of the hepatoduodenal ligament and slid inferiorly to the distal end for the examination of the CBD. The proximal part of CBD, left and right hepatic ducts and their junction were investigated through the right hepatic lobe. Diameter of the CBD and cystic duct, as well as size and number of stones, were measured for determining the choledochoscopy approach. The transcholedochal approach was chosen in cases where stones in CBD were larger than the obtainable diameter of cystic duct.
If transcholedochal approach was considered feasible, an incision was made on CBD longitudinally and the duct was flushed extensively with normal saline. Subsequently, a 2.5 mm flexible choledochoscope was inserted and bile ducts were examined distally and proximally under visual control. Stones were removed using baskets inserted through the instrument channel of the choledochoscope or using Fogarty (No. 3 or 4) catheters. After removal of all stones, clearance of the common bile duct was confirmed with choledochoscopic visualisation and repeated intra-operative ultrasound. CBD was closed primarily with interrupted 3-0 absorbable sutures, except for cases of severe cholangitis when T-tubes were inserted or choledocho-duodenostomy in cases of dilatation of common bile duct >15 mm.
The age and gender of the patients, preoperative comorbid conditions according to the ASA score, results of the preoperative imaging, and the status of inflammatory response including WBC count, CRP, liver enzyme levels and lipase activity, and presence of cholangitis were compared between groups. Diagnostic accuracy of the intraoperative US, success rate of the clearance of the CBD, magnitude of the inflammatory response, complication rate and main outcomes were the variables to compare treatment success.
Statistical analysis
Interval data was presented in median (Me) with interquartile range (IQR) and was confirmed by the Kolmogorov-Smirnov test for the asymmetrical distribution of data. Comparison of the interval data in CH+ and CH- groups was performed with the Mann-Whitney U test, the nominal data comparison performed using the Pearson χ2 test and Fisher's exact test. Significant dynamics of laboratory analysis were revealed by the Wilcoxon test. The correlation between hospital stay and clinical data was evaluated using the Spearman rho method. Also, the correlation coefficient was compared between groups. A logistic regression analysis was performed to identify factors associated with a longer hospital stay. A p-value <0.05 was considered as statistically significant. The statistical analysis was performed with SPSS version 20 and MedCalc version 15.
Ethics
The assessment and usage of all clinical data was approved and permitted before the study by the ethics committee of the Riga Stradins University. The study protocol conformed to the ethical guidelines of the "World Medical Association (WMA) Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects" adopted by the 18th WMA General Assembly, Helsinki, Finland, June 1964 and amended by the 59th WMA General Assembly, Seoul, South Korea, October 2008.11
Go to :
RESULT
Out of a total of 320 patients who underwent laparoscopic cholecystectomy and intraoperative US for suspected choledocholithiasis, 99 patients with intraoperatively confirmed choledocholithiasis underwent laparoscopic choledochoscopy and clearance of the CBD (Fig. 1). In this cohort, 60 patients had signs of cholangitis (CH+) and 39 had no signs of cholangitis (CH-) (Table 1, Fig. 1).
Preoperative findings
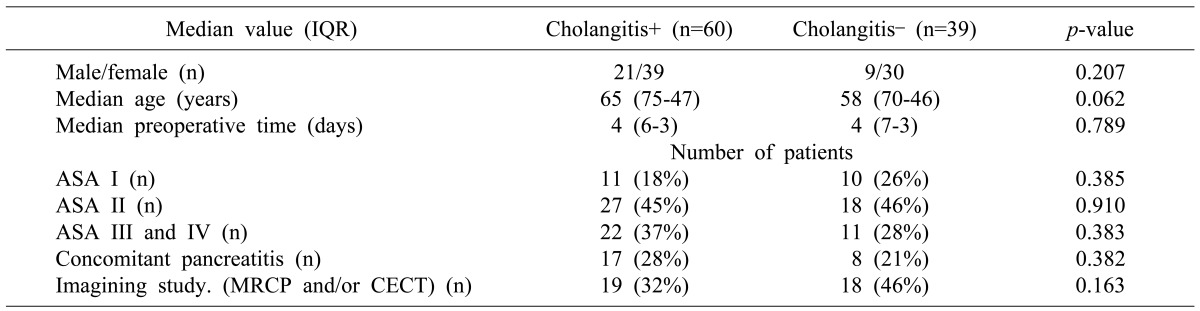
The incidence of comorbid conditions did not differ between the groups. Concomitant acute pancreatitis was observed in 28% of patients in the CH+ group without significant difference, as compared to the CH- group. Preoperative MRCP and CECT were conducted in 32-46% of patients without group wise difference. Preoperative preparation time was equal in both groups (Table 1).
Laparoscopy
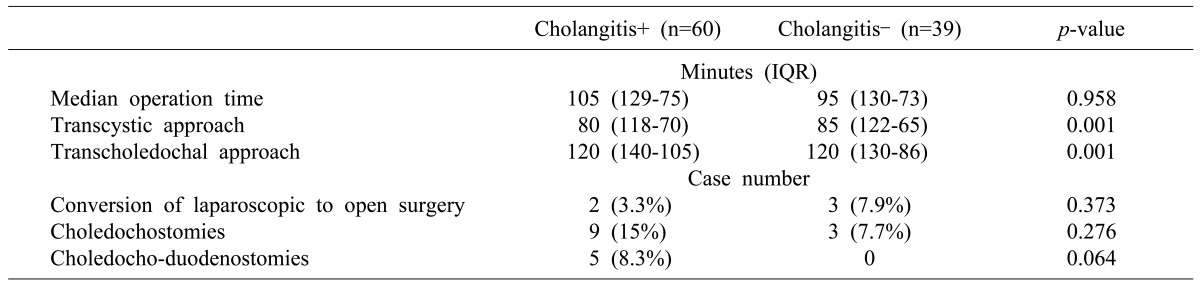
Both groups showed a total laparoscopic intervention time of 95-105 minutes and 3-7% conversion rate. Choledochoduodenostomies for cholangitis and dilatation of the common bile duct >15 mm, as well as most of the choledochostomies were performed the CH+ group. However, transcystic choledochoscopy was significantly shorter than the transcholedochal approach in both groups. Moreover, transcystic approach and transcholedochal approach had equal median procedure time between groups (Table 2).
Dynamics of inflammation
Preoperative inflammatory response was markedly higher in the CH+ group; however, liver enzyme levels, lipase activity and alkaline phosphatase were not different. Macroscopic signs of infection, inflammatory changes of the gallbladder and signs of the bile duct inflammation during the choledochoscopy were more evident in patients with cholangitis. Postoperative inflammatory response was not statistically different between groups (Table 3). The dynamics of C-reactive protein and white blood cell count were depicted in Figs. 2 and 3.
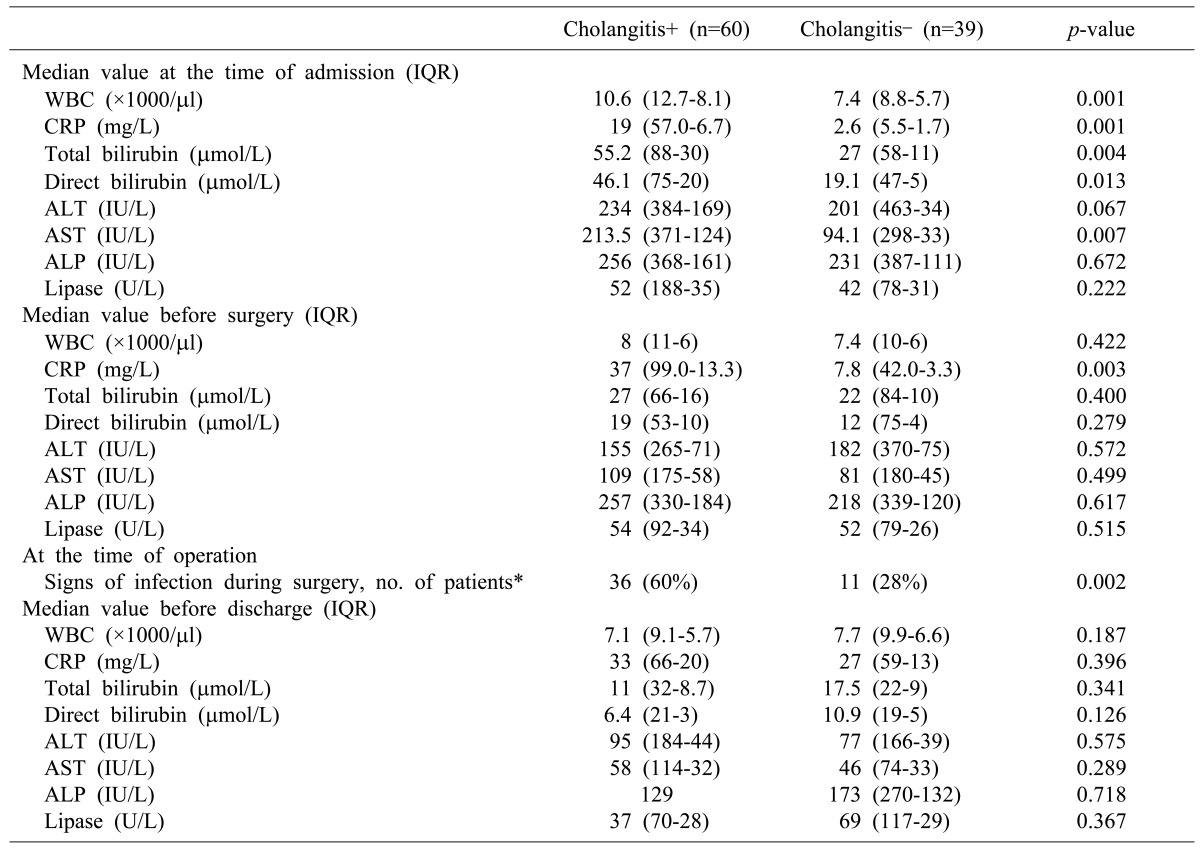
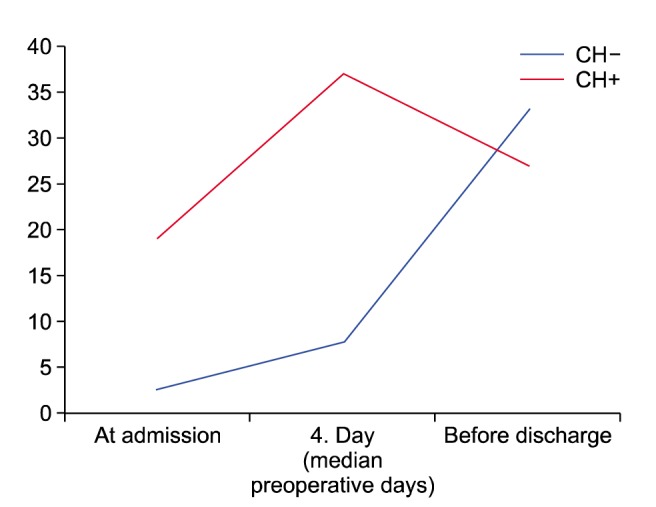
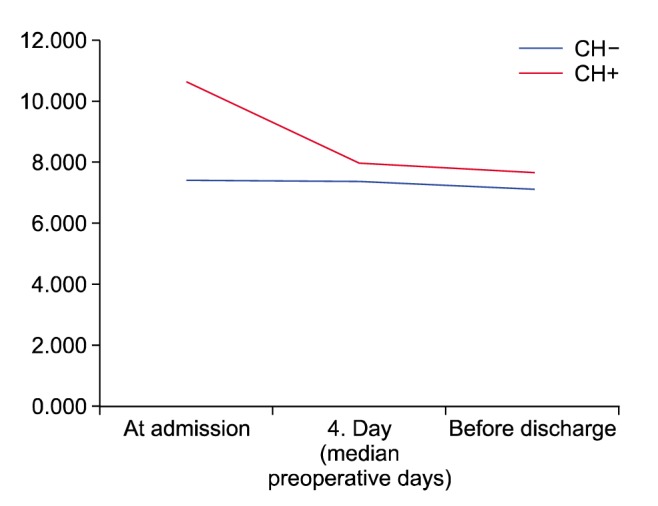
Table 3
Inflammatory response
WBC, white blood cell count; CRP, C-reactive protein; ALP, alkaline phosphatase; AST, aspartate aminotransferase; ALT, alanine aminotransferase. *Evidence of visible signs of acute cholecystitis during laparoscopy (histologically confirmed acute phlegmonous or gangrenous cholecystitis and/or empyema of gallbladder) and cholangitis during choledochoscopy (purulent or fibrinous bile)
![]()
Complication rate and outcomes
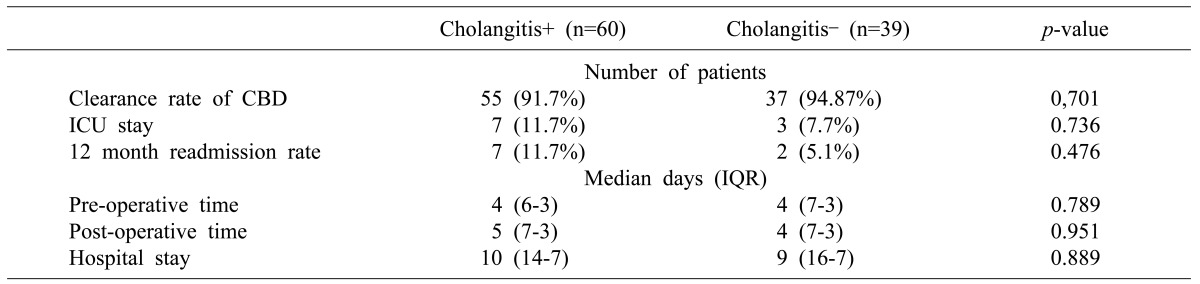
The overall complication rate reached 8.3%, including bleeding from the liver bed in 3 patients from the CH+ group, requiring surgical intervention in 1 patient, 1 bile leak and 1 case of pulmonary thromboembolism, treated conservatively. One patient from the CH- group required open surgery due to injury of the diaphragm and 1 was treated conservatively due to postoperative bile leak, comprising 5.1% of the group, p=0.701. Postoperative intensive care unit stay and overall hospital stay was not statistically different between groups. Laparoscopic clearance of the CBD was associated with 1 lethal case (CH+ group) due to decompensated liver cirrhosis and progressing hepatocellular insufficiency, resulting in 1% mortality rate in the cohort of 99 patients. A similar 12-month readmission rate was observed in both groups. Totally, complete laparoscopic clearance of the common bile duct was possible in 92.9% of patients (92 of 99); furthermore, the clearance rate was similar in both groups (Table 4).
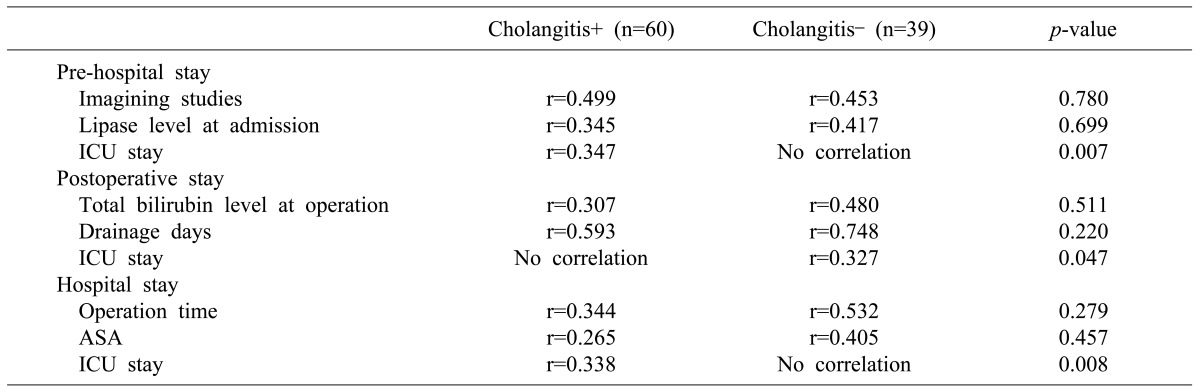
Correlation analysis
Correlation analysis revealed that patients with an elevated lipase level at the admission had a longer preoperative stay; and patients with an elevated total bilirubin level preoperatively had a longer postoperative stay. The duration of the operation and the severity of the comorbid conditions according to ASA score correlated with the overall hospital stay. Prolongation of the hospital stay was mostly associated with the presence of the comorbid conditions in the CH- group, p=0.001 (CI 95% 1.79-5.66) (Table 5).
Go to :
DISCUSSION
Preoperative recognition of the possible choledocholithiasis is crucial for planning of the treatment strategy in patients with a complicated course of gallstone disease. Existing recommendations for the management of patients with a complicated gallstone disease are controversial. Contrastenhanced computed tomography scan or MRCP is recommended as a routine preoperative radiologic examination with high sensitivity for patients with suspected bile duct involvement, especially when malignant lesions cannot be excluded.121314151617
However, MRCP may fail to visualise the sludge and stones <5 mm in diameter and bile duct stones in the cases of pancreatitis.118192021 The 2 recommended approaches include laparoscopic cholecystectomy with intraoperative evaluation of the CBD in the time of admission182223 or early ERCP, followed by delayed cholecystectomy 6-8 weeks later, especially for patients with acute pancreatitis.24 Evidence suggests that the results on ERCP treatment are more dependent on the selection of appropriate indications for ERCP and technical skills of the endoscopy specialist than on the patients' medical condition.2 Also, the reported mortality rate after cholecystectomy performed during the acute episode of biliary pancreatitis is higher.25
Contrary to a more routine concept of cholecystectomy in the interval after conservative treatment,24 several studies have demonstrated good results from laparoscopic cholecystectomy in index hospital admission during the acute phase of the disease.1822 The current study corroborated these results, with similar general patient characteristics (mean age, gender and comorbidities) and complication rate to those previously reported. This single-stage approach has become possible since the implementation of the intraoperative US visualisation of the CBD and choledochoscopy for the final clearing of the CBD when indicated.
The diagnostic value of the intraoperative US and the simplicity of performance has been demonstrated in several studies. It is currently a safe alternative to intraoperative cholangiography, excluding exposure to radiation and allowing a better anatomical visualisation.451926272829 According to the results of the current and similar studies, laparoscopic CBD clearance does not significantly increase the duration of the surgery, and is not associated with an increased complication rate. Moreover, intraoperative US control is especially effective in patients with infiltrated tissue and difficult visualisation of the biliary tree.1630 The conversion rate and reasons for conversion were not significantly different, but median operation time and post-operative stay were even shorter in both groups of our cohort, as compared with the experience from other studies.31
Thus, early laparoscopic clearance of the CBD following a single-stage strategy, is safe in patients with cholangitis, as recently reviewed.32 This strategy may reduce the risk of a recurrent attack and complications associated with delayed surgery. US visualisation and clearance of the CBD via transcystic or transcholedochal access requires better laparoscopic skills and more time spent in the operation theatre.33 This approach ensures postoperative control of CBD patency in patients with severe cholangitis or with incomplete clearance of the CBD, by adding T-tube drainage. It provides postoperative imaging of the biliary tree and for the removal of residual CBD stones and early postoperative ERCP when indicated. Alternatively to t-tube drainage, laparoscopic choledocho-duodenostomies might be created according to selective indications when dilatation of the CBD is >15 mm in elderly patients. Low 12-month readmission rate indicates that laparoscopic clearance of the CBD in emergently admitted patients is feasible, as previously reported.34
The lack of randomisation and a relatively long learning curve are the weak aspects of our study. Another weak point is the lack of a uniform protocol considering the preoperative standard of radiologic investigation, which was based on clinical, rather than scientific decision. However, single-stage laparoscopic interventions with provision of intraoperative US based choledochoscopic clearance of the CBD in emergently admitted patients resulted in a low complication rate and 1% mortality. The overall results and the low 12-month readmission rate indicated the safety and efficacy of this method.
We concluded that single-stage laparoscopic intraoperative US and choledochoscopy-assisted clearance of the CBD is feasible in emergently admitted patients with cholangitis. International prospective randomised study provided by specialists in the hepato-pancreatic-biliary surgery is justified to augment clinically based evidence.
Go to :
 XML Download
XML Download