

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Acute graft-versus-host disease (GVHD), a reaction of donor immune cells against host tissues, is a frequent complication (35%-50%) after allogeneic hematopoietic stem cell transplantation.1 In 1988, Burdick et al.2 first described acute GVHD after orthotopic liver transplantation (OLT). However, acute GVHD after liver transplantation is rare, occurring in 0.1%-2% of patients, but a severe complication with a 85% mortality rate in adult recipients.3456 Acute GVHD typically occurs 1-8 weeks after liver transplantation with symptoms of fever, diarrhea, and skin rashes in the early clinical course, followed by pancytopenia, sepsis, and even death.7 Currently, the correct diagnosis and management of GVHD following liver transplantation remain major challenges. Herein, we reported a patient with acute GVHD after liver transplantation that was successfully managed by withdrawal of immunosuppression.
Go to : 
CASE
Patient characteristics
A 47-year-old man with compensated hepatic cirrhosis due to a 28-year history of hepatitis B infection underwent OLT from a 19-year-old ABO-identical male donor after cardiac death in November 2013. The warm ischemic time and cold ischemic time were 5 minutes and 265 minutes, respectively. The recipient had severe complications of liver cirrhosis including hepatic encephalopathy and hypersplenism; and his Model for End-Stage Liver Disease (MELD) score was 30. Total blood loss during the surgery was 1956 ml, and the patient was given 8 units of red blood cells and 1000 ml plasma. Post-transplant immunosuppression regimens consisted of induction with anti-interleukin-2 receptor monoclonal antibody (basiliximab) followed by maintenance with steroids (methylprednisolone and prednisolone), tacrolimus (4.5 mg/d), and mycophenolate mofetil (750 mg, twice per day). The tacrolimus dose was adjusted to maintain the whole blood trough level at 8-12 ng/ml. Methylprednisolone and prednisolone were given at initial doses of 240 mg and 20 mg on postoperative day (POD) 1, respectively, and gradually tapered to 0 within 3 months. The postoperative course was uneventful, and the patient was discharged from the hospital approximately 3 weeks after surgery.
Acute GVHD after liver transplantation
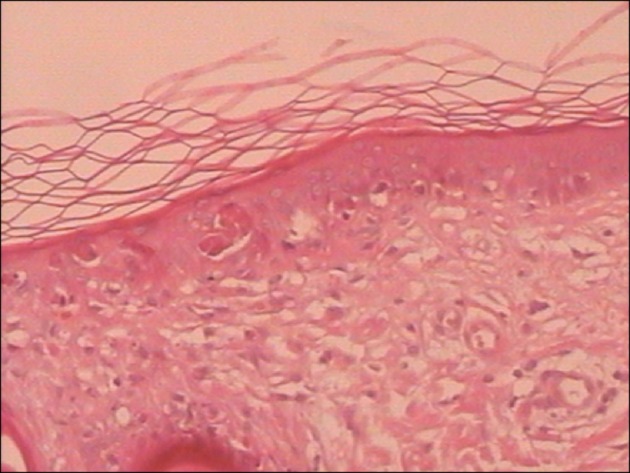
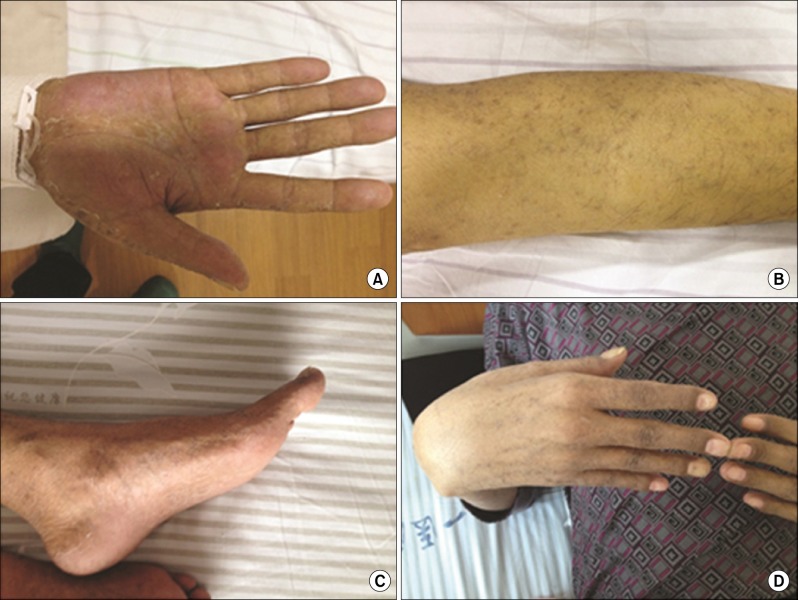
On POD 28, the patient developed a fever of 38.7℃, and he was treated with cephalosporin at a local hospital due to suspected bacterial infection. Unfortunately, the patient's condition deteriorated rapidly, and he showed signs of systemic inflammatory response syndrome (SIRS). He was then transferred to the intensive care unit in our hospital. On POD 29, the patient developed skin rashes on his limbs and trunk (Fig. 1A-C), and the rashes gradually spread to the whole body and integrated with each other. The patient also developed multiple oropharyngeal ulcers (Fig. 1D) and complained of dysphagia. The patient did not suffer from watery diarrhea during the entire clinical course. The blood tests showed that white blood cell (WBC) and platelet counts had dropped to 2.7×109/L and 22×109/L, respectively. Abdominal and chest computed tomography (CT) scans showed no positive findings. Cultures of blood, urine, and sputum for bacteria and viral serologic tests for cytomegalovirus (CMV) were all negative. A skin biopsy showed histological features consistent with GVHD (grade II), including focal liquefaction degeneration of the basal cells, scattered necrotic keratinocytes in stratum spinosum, and moderate lymphocytic infiltration in the dermis (Fig. 2).89 GVHD was suspected despite lack of chimerism of host- and donor-circulating lymphocytes among peripheral blood cells.

Because his fever did not improve, the patient was given cefmenoxime, cefoperazone/shuba tanner, meropenem, and teicoplanin to treat a possible bacterial infection, and fluconazole, caspofungin, and voriconazole for possible fungal infection. The immunosuppression therapy was gradually withdrawn, and only steroid (methylprednisolone, 2 mg/kg/day) was used in combination with gammaglobulin. Interleukin-11, colony-stimulating factors, and platelets were used for improving thrombocytopenia and promoting blood cell production. From POD 32, we noted a gradual disappearance of the skin rashes, followed by a decrease in temperature (36.5℃). On POD 35, the GVHD was finally confirmed by a skin biopsy and peripheral blood analysis employing fluorescence-activated cell sorting (FACS) and the immunosuppressive drugs including tacrolimus and mycophenolate mofetil were completely withdrawn. The plasma concentration of tacrolimus decreased to 0 on POD 38, and no immunosuppressive therapy was given between POD 35 and POD 42.
Drug-induced liver injury
On POD 42, the patient's aspartate aminotransferase (AST), alanine aminotransferase (ALT), total bilirubin (TBIL), and direct bilirubin (DBIL) levels were elevated to high levels (Fig. 3). Immunosuppressive drugs, included tacrolimus, mycophenolate mofetil, and high-dose methylprednisolone (500 mg/day for 3 days), were immediately used in the patient due to the risk of acute rejection. However, liver functions deteriorated despite these treatments, and the patient's clinical condition grew progressively worse. Thus, a liver biopsy was planned to explore the actual cause of abnormal liver function. The results of a subsequent liver biopsy were compatible with drug-induced liver injury (DILI, Fig. 4). On POD 53, rapamycin was used instead of tacrolimus, and drugs that might induce liver injury, such as meropenem, teicoplanin, and caspofungin, were withdrawn. The artificial liver support system was implemented in the patient to treat hepatic insufficiency on POD 55 and POD 59. Another liver biopsy was performed on POD 64, which confirmed the recovery of the liver from drug-induced injury. The patient was discharged with satisfactory clinical outcomes on POD 86 (Fig. 5).
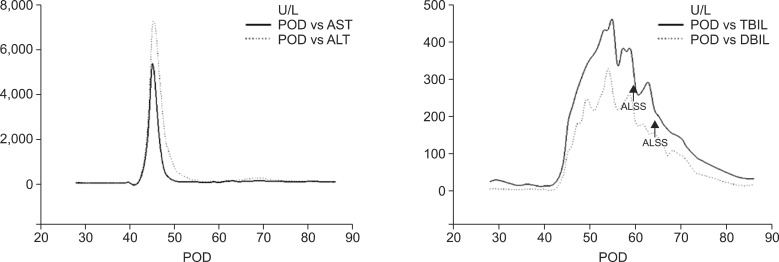 | Fig. 3Clinical course and laboratory changes following liver transplantation. (A) Serum AST and ALT concentrations during the postoperative period, (B) serum TBIL and DBIL concentrations during the postoperative period. ALSS, artificial liver support system; AST, aspartate aminotransferase; ALT, alanine aminotransferase; TBIL, total bilirubin; DBIL, direct bilirubin.
|
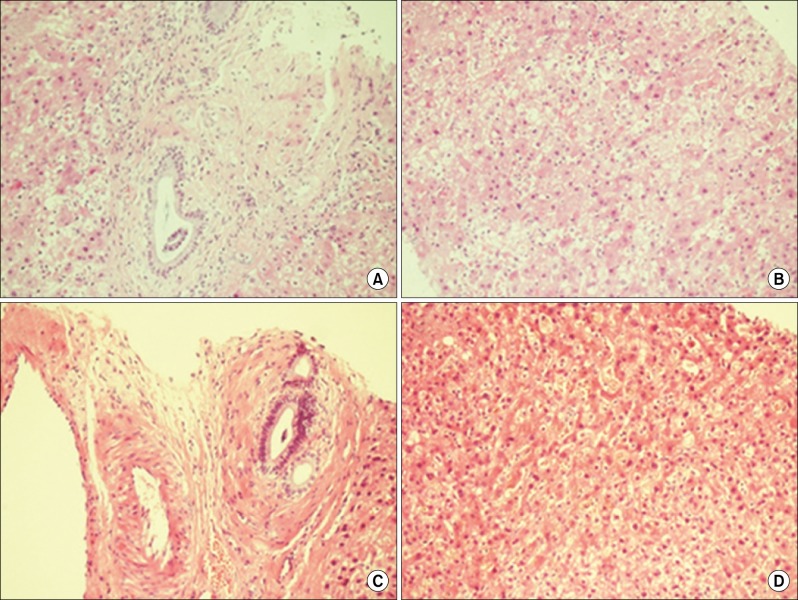 | Fig. 4Liver biopsy findings (H&E ×200). (A) Periportal infiltration of a few periportal neutrophils and lymphocytes at POD 50, (B) zone 3 cholestasis and lobular hepatocyte necrosis consistent with DILI at POD 50, (C) periportal infiltration of extremely few lymphocytes at POD 64, and (D) zone 3 cholestasis and lobular hepatocyte necrosis, eosinophilic bodies, and liver cell proliferation at POD 64.
|
Go to :
DISCUSSION
Acute GVHD following OLT is a rare but fatal complication that poses both diagnostic and therapeutic challenges. Usually, the diagnosis of acute GVHD is based on the presence of clinical manifestations and histopathological evidences.510 In the present case, the patient was readmitted 4 weeks after liver transplantation, presenting with symptoms of fever, skin rashes, decreased blood cell counts, and other typical signs of acute GVHD. The patient was finally diagnosed with acute GVHD by skin biopsy. In addition, earlier testing for chimerism by identifying donor's HLA antigen may lead to an earlier diagnosis of GVHD.6 The donor's HLA typing can be detected by polymerase chain reaction (PCR)-sequence-specific primers.31112 However, chimerism of host- and donor-circulating lymphocytes was not observed among peripheral blood cells in this case. One reason is that chimerism usually peaks in the first week, declines rapidly thereafter, and is usually absent beyond 3-4 weeks post transplantation, as reported by Taylor et al.1314
Currently, most therapeutic modalities for acute GVHD are based on GVHD management after hematopoietic stem cell transplantation and focus on increasing immunosuppression. However, this treatment does not demonstrate any survival benefit.315 Thus, some investigators have proposed reducing and even completely withdrawing immunosuppression as a treatment for GVHD after liver transplantation.3 Lehner et al.16 reported successful salvage treatment of acute GVHD in a liver allograft recipient by withdrawal of immunosuppression; they presented evidence that withdrawal of immunosuppressive therapy allowed the patient's immune system to reconstitute itself, reject offending lymphocytes, and avoid lethal septic complications. Our experience showed that a patient with acute GVDH can benefit from the novel therapeutic regimen including a high-dose of steroid, withdrawal of immunosuppression, and supplementation with gamma globulin.
In this case, when the patient discontinued the immunosuppressive drugs, he experienced elevations in the liver function tests. We first considered an acute rejection episode. However, the patient did not exhibit any improvement even after resuming immunosuppression. A subsequent liver biopsy helped to make a timely diagnosis of DILI. DILI is liver injury caused by various medications, leading to abnormalities in liver tests or liver dysfunction.17 The clinical presentation of DILI is highly variable from asymptomatic, reversible elevation of liver enzymes to fulminant hepatic failure.18 The diagnosis of DILI is difficult in patients with chronic liver disease and in those taking multiple potentially hepatotoxic drugs.17 In this case, all drugs that might induce liver injury were immediately withdrawn from the patient at the time of diagnosis of DILI. In addition, we used artificial liver support system to provide temporary support of liver function for the patient with success.
In conclusion, withdrawal of immunosuppression may serve as an effective treatment for acute GVHD after liver transplantation. During treatment, in addition to acute rejection episodes, awareness of drug-induced liver injury is necessary if the results of liver function tests are elevated, especially for patients taking multiple potentially hepatotoxic drugs, such as broad-spectrum antibiotics.
Go to :
 XML Download
XML Download