

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Intraductal papillary neoplasms of the bile duct (IPNB) have been associated with papillary tumors of malignant potential in the extrahepatic and intrahepatic bile ducts.123 IPNB is classified as a distinct clinical and pathological entity in the 2010 World Health Organization classification.4 Its malignant potential reportedly ranges from 19.5% to 83%.5 These tumors show papillary proliferation in the bile duct with or without mucin secretion and are considered as IPNB, the biliary counterpart of intraductal papillary mucinous neoplasm (IPMN) of the pancreas.467
Some mucin-producing IPNBs can cause obstructive jaundice due to production of abundant high-viscosity mucin.4 Herein, we presented two cases of mucin-producing IPNBs with obstructive jaundice who underwent resection of the intrahepatic primary lesions and bypass hepaticojejunostomy.
Go to : 
CASE
Case 1
A 69 year-old male was admitted to the emergency room due to obstructive jaundice. Five years ago, he underwent lung resection for adenosquamous carcinoma of the lung, without recurrence to date. At the time of lung surgery, he was diagnosed with gallbladder stones and hepatolithiasis of the segment III, VI and VIII ducts (B3, B5 and B8) with corresponding ductal dilatation, suggestive of associated inflammatory stricture. Yearly imaging study follow-up for gallstone lesions until the recent last visit to emergency room showed no interval changes of gallstone disease or evidence of malignant changes.
Imaging study findings of dynamic liver computed tomography (CT) and magnetic resonance (MR) imaging were as follows: mucin-secreting IPNB mainly in B3 with slight interval aggravation of biliary ductal dilatation; and multiple intrahepatic duct stones, interval increased extent and gallbladder (Fig. 1A and 1B). Cancer Antigen 19-9 (CA 19-9) was mildly elevated (38 U/ml). Endoscopic retrograde cholangiography (ERC) showed multiple filling defects in the biliary system, which was compatible with mucin-producing IPNB (Fig. 1C and 1D). Two endoscopic nasobiliary tubes were inserted and retained for 10 days in order to mediate biliary decompression.
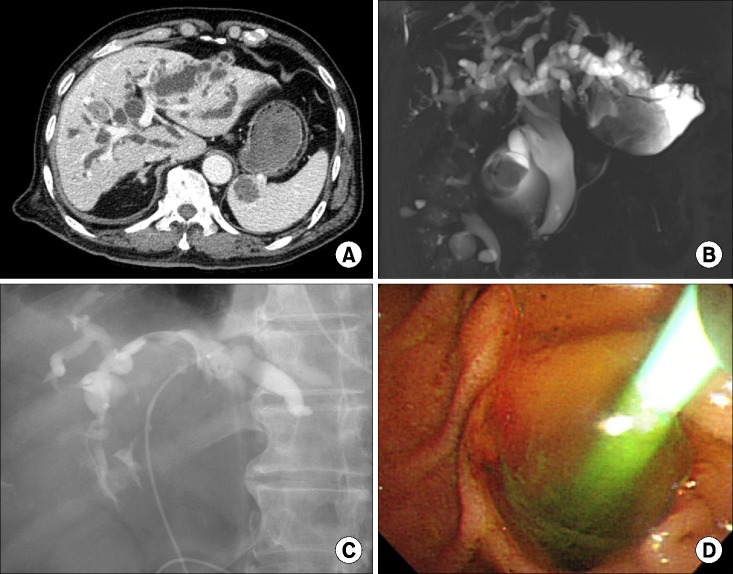 | Fig. 1Preoperative imaging study findings of Case 1. (A) Computed tomography image shows diffuse dilatation of the intrahepatic duct and stones; (B) Magnetic resonance cholangiography shows markedly dilated intrahepatic ducts filled with mucin and stones; (C) Endoscopic retrograde cholangiography shows filling defects at the intrahepatic ducts and common bile duct; and (D) Endoscopic retrograde cholangiography shows high-viscosity mucin drainage from the ampulla of Vater.
|
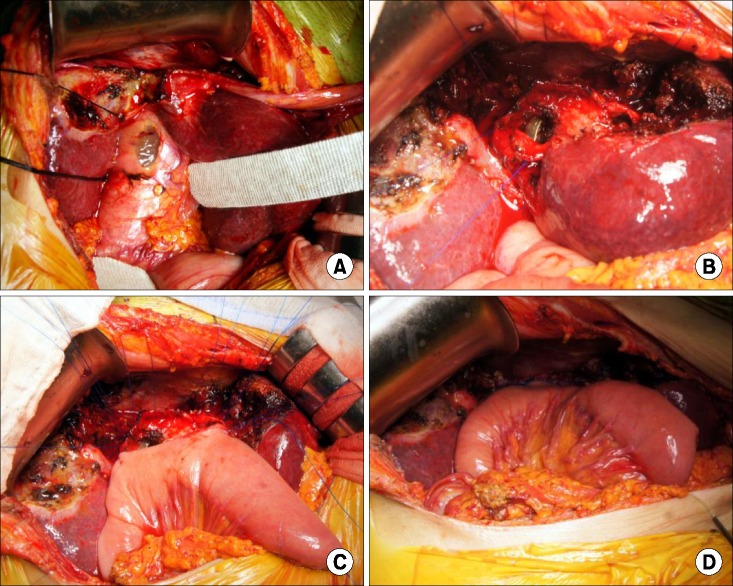
After laparotomy, we first opened the fully distended common bile duct (Fig. 2A and 2B). After removing the very sticky mucin, the B3 cystic lesion identified as the source of the mucin was excised and a 2 cm-sized B3 opening was exposed (Fig. 2C and 2D). Frozen-section biopsy revealed that the B3 cystic wall was involved with cancer, thus the whole B3 duct wall except its connecting part to the left intrahepatic duct was resected. Intrahepatic duct stones at B5 and B8 were removed with curved stone forceps. Due to some risk of residual tumor that could re-induce mucin production, we performed two separate biliary bypass drainages to the common bile duct and B3 orifice (Fig. 2E and 2F). The operation included segment III hepatic resection, intrahepatic stone removal, end-to-side choledochojejunostomy and B3 hepaticojejunostomy.
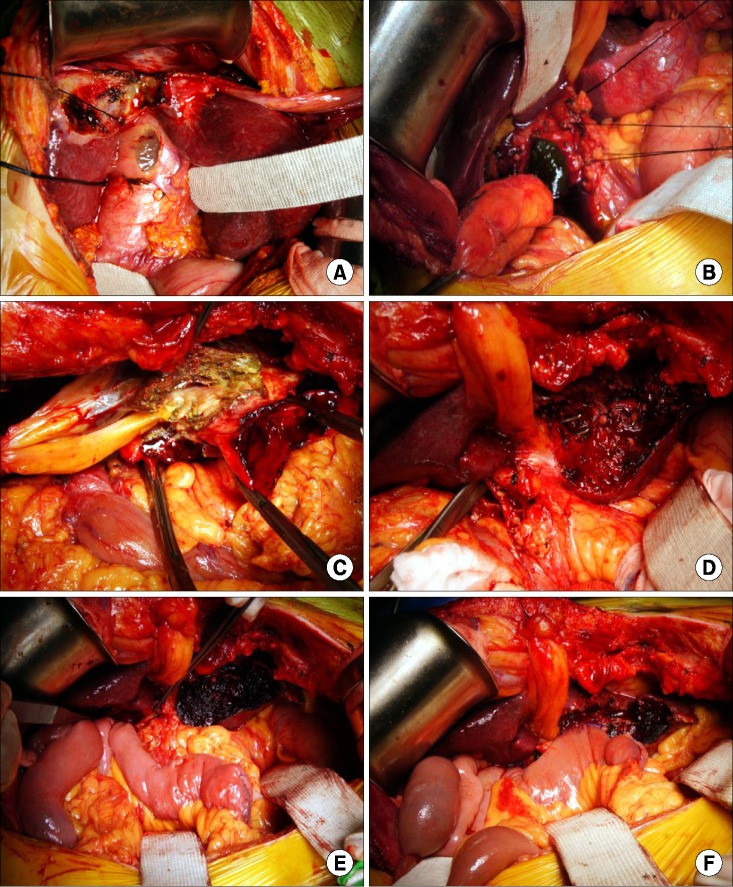 | Fig. 2Operative photographs of Case 1. (A) At laparotomy, the segment III cystic lesion is protruded; (B) The common bile duct is filled with mucin; (C) The segment III cystic lesion is dissected from the hepatic parenchyma; (D) The segment III cystic lesion is excised; (E) Endto-side choledochojejunostomy is performed; and (F) B3 hepaticojejunostomy is completed.
|
Pathologic findings were as follows: intrahepatic cholangiocarcinoma with intraductal growth type; confinement to bile duct wall; no lymphovascular invasion; no perineural invasion: no involvement of B3 margin and hepatic parenchymal resection margins; biliary intraepithelial neoplasia 2 at the common bile duct wall; and chronic cholangitis with bile duct dilatation, extensive erosion, multifocal rupture and abscess and xanthogranulomatous inflammation.
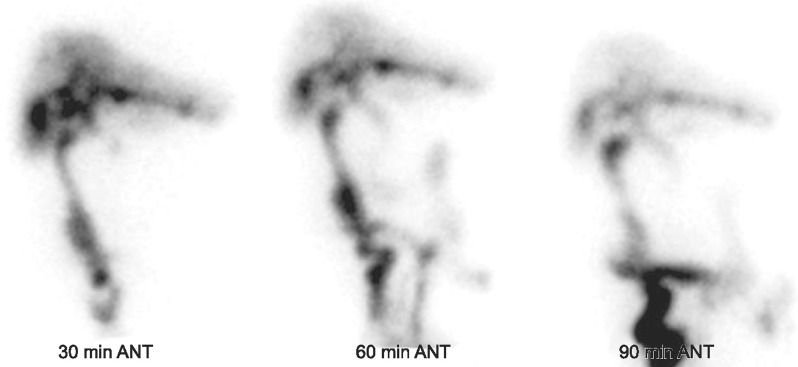
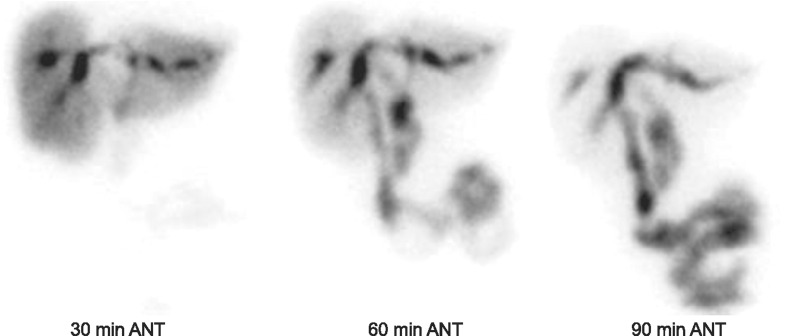
The patient recovered uneventfully from surgery. Follow-up hepatobiliary scintigraphy showed uneventful biliary drainage (Fig. 3). Since this resection was regarded as R0 resection, no additional adjuvant treatment was scheduled. He has been doing well for 6 months post-surgery.
Case 2
A 74 year-old female was referred for surgery due to suspected malignant mucin-producing IPNB and obstructive jaundice. She had undergone repeated episodes of ERC and percutaneous transhepatic cholangiography (PTC) for recurrent intrahepatic and common bile duct stones for the last 11 years.
Findings of dynamic liver CT and MR imaging were as follows: mucin-producing IPNB with asymmetric disproportional dilatation in the segment IV duct (B4) and mural nodule in B4; increased fluid collection due to bile duct rupture at the right subphrenic space adjacent to the segment IV (Fig. 4A and 4B). Chest CT and positron emission tomography showed multiple mild hypermetabolic lymph nodes in right internal mammary chain, suggesting metastatic lymph nodes. CA 19-9 was mildly elevated (52 U/ml).
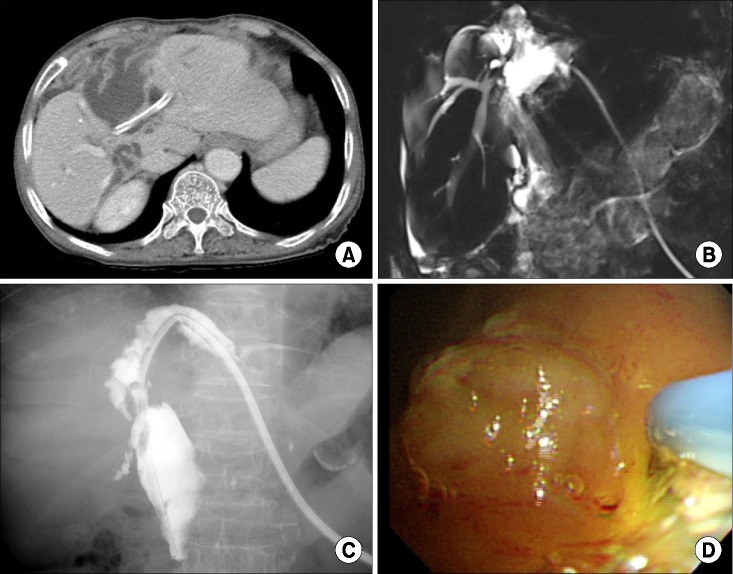 | Fig. 4Preoperative imaging study findings of Case 2. (A) Computed tomography image shows a cystic dilatation at the segment IV; (B) Magnetic resonance cholangiography shows markedly dilated left intrahepatic ducts filled with mucin; (C) Percutaneous transhepatic biliary drainage shows filling defects at the left intrahepatic ducts and common bile duct; and (D) Percutaneous transhepatic cholangioscopy shows high-viscosity mucin within the left intrahepatic duct.
|
PTC was performed for biliary decompression and tissue confirmation; intra-operatively, the intraductal mass was diagnosed as IPNB of intermediate grade dysplasia (Fig. 4C and 4D).
After laparotomy, we first opened the fully distended common bile duct (Fig. 5A). After removing the very sticky mucin, the B4 cystic lesion identified as the source of mucin was excised and two 3 cm-sized right and left hepatic duct openings were exposed (Fig. 5B). Frozen-section biopsy revealed that the B4 cyst wall was involved with cancer. We decided to perform non-curative resection since residual scattered bile duct tumors at the hepatic confluence portion did not permit simple resection and left hepatectomy was contra-indicated due to patient safety.
 | Fig. 5Operative photographs of Case 2. (A) The common bile duct is filled with mucin; (B) The segment IV cystic lesion is excised; (C) Two large openings to the right and left hepatic ducts are unified with running sutures and then reconstructed with single large hepaticojejunostomy; and (D) Central hepaticojejunostomy is finished.
|
Due to high risk of residual tumors that could re-induce mucin production, these lesions were destroyed with deep electrocautery and argon beam coagulator. We also decided to perform biliary bypass drainage. Two large openings to the right and left hepatic ducts were unified with running sutures and then reconstructed with single large hepaticojejunostomy (Fig. 5C and 5D). The longitudinal incision at the common bile duct was securely repaired. The operation included segment IV hepatic resection, partial resection of the diaphragm and central hepaticojejunostomy.
Pathologic findings were as follows: well differentiated mucinous adenocarcinoma of nodular type arising from IPNB; extension beyond bile duct; serosal penetration and involvement of the diaphragm; no lymphovascular invasion; no perineural invasion; involvement of the radial resection margin; and no involvement of common and hepatic bile duct resection margins.
The patient recovered uneventfully from surgery. This resection was regarded as R1/R2 resection with possibility of distant lymph node metastasis, but no additional adjuvant treatment was planned due to poor general condition of the patient. Follow-up hepatobiliary scintigraphy showed uneventful biliary drainage (Fig. 6). She has been doing well for 4 months post-surgery without any evidence of tumor recurrence or distant metastasis.
Go to :
DISCUSSION
IPNB is considered a precursor lesion of cholangiocarcinoma.12 IPNB was proposed as a new disease entity because of striking similarities to IPMN of the pancreas, wherein the disease entity and clinicopathological features are well established.8 However, preoperative diagnosis of intrahepatic IPBN is usually difficult in practice. The common clinical manifestations of patients with intrahepatic IPNB are recurrent abdominal pain, repeated episodes of acute cholangitis and obstructive jaundice, as presented in our previous study.1
Intrahepatic duct dilatation and intraductal mass are common abnormal findings in patients with intrahepatic IPNB. Cholangiography, including indirect cholangiography (MR cholangiography) and direct cholangiography (ERC and PTC), is useful to show the entire bile duct to define the extent of the IPNB.910 Mucin cannot be detected on usual imaging studies. Direct cholangiography is useful for the detection of mucobilia.8 However, ERC and PTC are invasive procedures, which not only risk introducing bacteria into the bile duct, but more importantly may result in dissemination of tumor cells. Mucinous obstruction of bile duct prevents visualization of the whole biliary tree as well as tumor detection by cholangiography. PTC and ERC are usually performed in patients with obstructive jaundice, but it is often not possible to relieve the jaundice by draining the inspissated mucobilia.10
Cholangioscopy including percutaneous transhepatic cholangioscopy (PTCS) and peroral cholangioscopy can approach the bile duct directly, confirm the histology, and assess the extent of the tumor including superficial spreading along the biliary epithelium, which facilitates appropriate treatment choice.58 We prefer PTCS to peroral cholangioscopy for reliable evaluation of the intrahepatic duct in patients with mucin-producing lesions; in addition, percutaneous transhepatic biliary drainage enables biliary decompression in the environment of sticky mucin formation. PTCS examination is therefore an indispensable preoperative procedure for determining treatment modality and the appropriate extent of resection in intrahepatic IPNB.111
Intrahepatic IPNB should not be regarded as a benign disease with low malignant potential but as a premalignant lesion with high malignant potential. In our previous study, low-grade intrahepatic IPNB was rather rare and the majority of intrahepatic IPNB cases were high-grade IPNB, and invasive IPNB with minimal and considerable invasion.1 IPNB with different malignant potentials can be ultimately diagnosed as adenoma, borderline tumor, non-invasive carcinoma or invasive carcinoma,12 a continuum of intraductal neoplastic progression.
IPNB has many similarities to pancreatic IPMN. In both organs, these neoplasms arise within the ductal system and show a predominantly intraductaI growth pattern macroscopically and papillary proliferation with delicate fibrovascular cores.1314 Their pathological similarities are summarized as follows: macroscopic growth pattern of intraductal papillary proliferation; occasional association with mucin hypersecretion; microscopic feature of papillary proliferation with fibrovascular cores; occurrence of three types of tumor cells; occasional association with multiple lesions; possible progression to tubular adenocarcinoma and mucinous carcinoma; and influence of histological types of invasive lesion on survival rate. Their pathological differences are summarized as follows: high frequency of CK20 expression in IPNB than in pancreatic IPMN; lower percentage of gastric type tumors in IPNB than in pancreatic IPMN; and lower frequency of mucin hypersecretion in IPNB than in pancreatic IPMN.14
Mucin is macroscopically identifiable in most cases of pancreatic IPMN but in only less than one-third of IPNB cases.61516 We previously reported that mucin pool formation was observed in only 7 of 43 cases (16.3%).1 Mucin-producing IPNB is capable of secreting abundant quantities of mucus. The liquid is colorless, ropy, and has a viscous consistency. The liquid is composed of mucin and albumin and is rich in electrolytes, but contains neither bile salts nor pigments. Its external drainage is often contraindicated because it is followed by discharge of extraordinary quantities of mucobilia and leads to marked loss of proteins and electrolytes.17
Because patients with intrahepatic IPNB often show favorable prognosis, curative surgical resection is regarded as the first-choice treatment for patients with intrahepatic IPNB without distant metastasis. Early and accurate diagnosis is therefore important in this disease entity. We previously showed that surgical curability was the only reliable prognostic factor for tumor recurrence and patient survival.1
Palliative treatments are recommended if curative resection is not feasible.17 Especially in patients with mucin-producing tumors, hepaticojejunostomy can palliate the liquid loss and is also efficient, at least temporarily, in previously reported cases.18
In this study, the 2 patients were diagnosed with intrahepatic stone disease 5 and 11 years prior to surgery, respectively. They had been observed or managed with interventional treatment for a long time. It is likely that the pre-existing dysplastic lesions transformed to malignancy at a certain time, resulting in acceleration of mucin production. They were referred for surgical treatment only after obstructive jaundice was developed due to massive mucin production. In retrospect, closer follow-up may have led to earlier surgical treatment and better outcome, but poor general condition of these patients did not lead to surgery before manifestation of overt symptoms. The long-term clinical courses of our patients highlight that abundant production of highly viscous mucin might be associated with malignant transformation.
In conclusion, we presented two rare cases of mucin-producing IPNB of malignant transformation that were treated with primary resection and biliary drainage. The case studies indicated that abundant production of highly viscous mucin inducing obstructive jaundice may be associated with malignant transformation in patients with IPNB.
Go to :
 XML Download
XML Download