

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Sinusoidal obstructive syndrome (SOS) was initially called veno-occlusive disease,1 based on the triad of jaundice/hyperbilirubinemia (>2 mg/dl), painful hepatomegaly and ascites/weight gain. It is confirmed by the histologic findings of fibrous obliteration of small hepatic veins by connective tissue and centrilobular hemorrhagic necrosis.2 The most frequent cause of SOS is the use of high-dose chemotherapy in recipients of hematopoietic stem cell transplantation.345 SOS is also described after liver transplantation (LT), but with relatively rare occurrence of approximately 2%.6 Severe SOS leads to mortality rates of 84-90%.78 Development of SOS after LT is reportedly associated with tacrolimus administration.9 Herein, we described a case of SOS following stenosis of the inferior vena cava after living donor liver transplantation (LDLT).
Go to : 
CASE
A 34-year-old woman with hepatitis B virus-associated liver cirrhosis with model for end-stage liver disease score of 15 underwent LDLT operation using a right lobe graft from a 27-year-old living donor in 2015. The cold and warm ischemic times were 130 minutes and 80 minutes, respectively. Serum total bilirubin increased to 25.4 mg/dl until post-operation day (POD) 7, and Gamma glutamyl transpeptinase (GGT) 248 mg/dl at POD 13. Doppler ultrasonography indicated the right hepatic vein (RHV) outflow rate of 37 cm/sec and enhanced computed tomography (CT) at POD 14 revealed no vascular abnormality. Thereafter, the patient condition was stabilized.
Repeat CT scan at POD24 revealed biloma around the liver graft (Fig. 1A). The laboratory profiles showed decrease in total bilirubin to 1.6 m/dl, but increase in C-reactive protein (CRP) to 129 mg/dl. Abdominal drainage culture was Escherichia coli-positive; therefore, antibiotic was changed to Meropenem. Thereafter, CRP decreased to 3.9 mg/dl and CT scan at POD 33 showed normal liver findings. The patient was discharged from the hospital. Blood tacrolimus level was maintained around 10-14 ng/ml during the hospitalization.
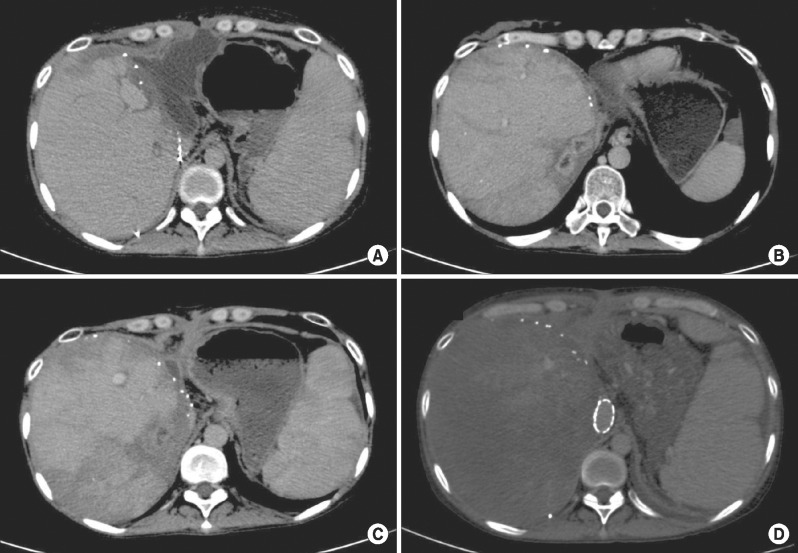 | Fig. 1Sequences of computed tomography (CT) findings: (A) CT scan shows biloma around the liver graft; (B) CT scan taken at day 73 shows multifocal liver abscesses; (C) CT scan shows treatment of liver abscess following antibiotics therapy; and (D) CT scan shows that the liver parenchyma was undefined after stenting of the inferior vena cava.
|
At POD 73, she complained of high fever and upper abdominal discomfort. Laboratory study showed CRP 47.4 mg/dl and white blood cell count 3890/µl, and tacrolimus level 15-20 ng/ml. Doppler ultrasonography showed RHV outflow rate 30 cm/sec; and CT scan showed multifocal liver abscesses (Fig. 1B). On admission, she received antibiotic and supportive therapy. The size of liver abscess decreased after 9 days (Fig. 1C) and the patient was discharged at POD 83.
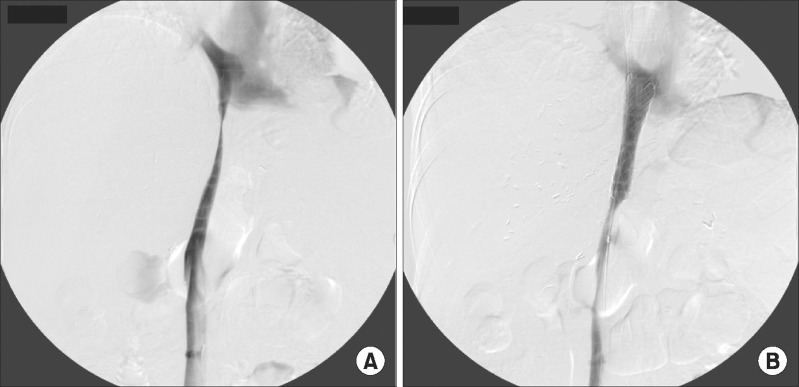
After 6 months, she complained of foot edema and ascites. CT scan revealed stenosis of the retrohepatic inferior vena cava (IVC), thus direct angiography was performed (Fig. 2A). At that time, the liver function profiles were not impaired: total bilirubin 1.1 mg/dl; aspartate aminotransferase (AST) 18 IU/L; alanine aminotransferase (ALT) 10 IU/L; GGT 31 IU/L; alkaline phosphatase (ALP) 100 IU/L; and creatinine 0.6 mg/dl. To resolve IVC stenosis, an IVC stent (Hercules Vascular Stent, S&G Bio Tech: Seongnam-si, Korea) was inserted without any noticeable complication (Fig. 2B).
However, after IVC stenting, she started to complain of abdominal discomfort. The liver function was impaired: total bilirubin 11.5 mg/dl; AST 698 IU/L; ALT 317 IU/L; GGT 42 IU/L; ALP 120 IU/L; and creatinine 2.35 mg/dl. Doppler ultrasonography showed significant decrease in RHV flow rate to 13 cm/sec after IVC stenting; and CT scan 9 days after stenting showed non-enhancement of the liver parenchyma (Fig. 1D). The patient's condition continued to worsen with aggravating jaundice, ascites, and hepatic encephalopathy. Finally, 8 months after LDLT, she underwent retransplantation with a deceased donor liver graft. The patient's condition was critical (total bilirubin 31.8 mg/dl; AST 42 IU/L; ALT 9 IU/L ; GGT 43 around the portal tracts. IU/L; ALP 513 IU/L; and creatinine 0.95 mg/dl; INR 3.72). The retransplantation operation was complex and took 15 hour 20 min due to patient's condition and abdominal adhesion. Blood loss was massive and we were unable to control the leakage of blood when closing the abdominal incision. After the operation, she continued in critical condition (total bilirubin 4.7 mg/dl; AST 1555 IU/L; ALT 269 IU/L ; GGT 15 IU/L; ALP 23 IU/L; and creatinine 1.06 mg/dl; INR 1.94). The patient was intubated for 9 days post-operatively, and showed gradual improvement. Her blood tacrolimus level was maintained around 10-14 ng/ml during the hospitalization.
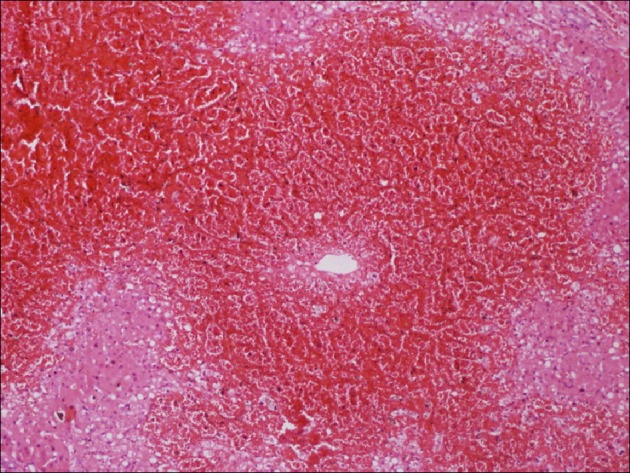
The explant liver pathology was consistent with SOS (Figs. 3 and 4). Microscopic examination suggested SOS, characterized by massive venous congestion, replacement of parenchyma with blood, and a few surviving hepatocytes around the portal tracts.

Go to :
DISCUSSION
SOS is characterized by toxic injury of sinusoidal endothelial cell, which is revealed as loss of sinusoidal wall. SOS is occasionally associated with perisinusoidal fibrosis, centrilobular hepatic vein fibrotic obstruction, nodular regenerative hyperplasia, and peliosos.10 The incidence of clinical SOS after LT is reported to be 1.9-2.9%.1112 The clinical signs and symptoms are non-specific after LT, which results in difficult and complicated diagnosis. Developing SOS after LT reportedly correlates with acute cellular rejection.5 An in vitro study showed that toxins and drugs that cause hepatic SOS are more toxic to the hepatic sinusoidal endothelial cells than to the hepatocytes.1314
Our present case was diagnosed based on explant pathology after retransplantation. The precedent underlying cause of SOS was possibly graft liver abscess and subsequent IVC stenosis. This case was not associated with any episode of acute rejection and we could exclude other potential pathology as well as infectious complication. Moreover, the explant liver pathology showed 25% macrovesicular steatosis. A specific polymorphism of the glutathione-S-transferase gene is found more frequently among patients with SOS.15 Thrombotic microangiopathy associated with significantly reduced survival following the allogeneic hematopoetic stem cell transplantation is another risk factor for development of transplantation-associated SOS.16 Also, evidence of clotting abnormalities in the experimental model of hepatic SOS is lacking.17
In particular, cytomegalovirus infection mediated vascular injury, results in incidence of hepatic artery thrombosis after LT. This injury occurs in the sinusoidal endothelium, which increases the risk of SOS development. Positive expression of cytomegalovirus infection was absent in our case.
Tacrolimus is primarily metabolized by the cytochrome P450 (CYP) 3A subfamily in liver microsomes. The zone 3 of the liver acinus has the highest levels of CYP and is the most affected by SOS.18 Hence, we considered Tacrolimus a potential factor for development of SOS after LT in our case. However, its 24-hour trough level was maintained between 10-16 ng/ml, which suggested no association with SOS development.
In conclusion, the underlying causes of SOS are a complex pathologic entity with multifactorial etiology. Its multifactorial etiologies are likely to include a decrease of hepatic venous outflow that is caused by graft liver infection and IVC stenosis.
Go to :
 XML Download
XML Download