

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Pancreatic neuroendocrine tumors (NETs) are rare neoplasms that arise in the endocrine tissues of the pancreas and account for <3% of all primary pancreatic tumors.12 Most pancreatic NETs are sporadic, but may be associated with hereditary endocrinopathies. The reported annual incidence ranges between 0.32–0.43/100.000, but has risen recently due to increased detection of asymptomatic disease on cross-sectional imaging.23 The majority are non-functional and present with non-specific symptoms or are asymptomatic. Peptide hypersecretion from pancreatic NETs occasionally presents with a hormonal syndrome.456 In general, they are associated with relatively good survival, although significant variability in outcomes may be seen, based on biological heterogeneity.456
Functional status, tumor localization, histological grade and TNM classification are all important factors determining treatment strategy. Small (<1-2 cm) locoregional, well-differentiated tumors with favourable imaging characteristics, have low metastatic potential and surgical resection alone usually offers excellent results.78910
Conventional thermal ablative techniques such as radio-frequency ablation (RFA) and microwave ablation (MWA) can be used to treat pancreatic tumours, but there is a risk of thermal injury to the pancreatic duct and surrounding structures including the superior mesenteric artery (SMA), superior mesenteric vein (SMV), and duodenum.
Irreversible electroporation (IRE) is a novel non-thermal ablative therapy that is used primarily for treating liver tumors and pancreatic adenocarcinomas not amenable to resection or conventional ablation due to close proximity to major vascular or vital structures such as the bile duct or the pancreatic duct.11 Its principle is based on the delivery of short-pulsed high-voltage electric current through electrodes positioned adjacent to the tumor causing irreversible injury to cell membrane and cell death by apoptosis.11 For tumors located in the pancreas, it has been used for treatment of the non-metastatic locally advanced ductal adenocarcinoma following Folfirinox neoadjuvant chemotherapy and/or radiation, with the intention of achieving disease control.1213
Experience with this technique is available for locally advanced pancreatic cancer, but currently no available data exists on Medline for the use of IRE in pancreatic NETs. We presented 3 patients with one functioning and 2 non-functioning pancreatic NETs treated with IRE and discuss potential indications, complications and outcomes of this modality.
Go to : 
MATERIALS AND METHODS
Between April 2014 and March 2015, 3 patients underwent IRE for pancreatic neuroendocrine tumors (Table 1). The first patient presented with frequent hypoglycaemic episodes, elevated serum insulin but normal C-peptide (636 pmol/L range 298-2350). Computed tomography (CT) and magnetic resonance imaging (MRI) showed a 9 mm-sized enhancing lesion at the head of the pancreas consistent with NET (Fig. 1A). Octreotide scan was negative and endoscopic ultrasonography (EUS) with fine needle aspiration (FNA) of the lesion was performed. Histology showed features of NET, but due to insufficient sample, tests for NET markers or mitotic index were not done. A diagnosis of benign insulinoma was made, and conservative management with observation was offered in the first instance. The tumor remained stable over a period of 10 months, but the symptoms persisted. Treatment options including IRE were discussed with the patient and a decision was made to proceed with IRE.
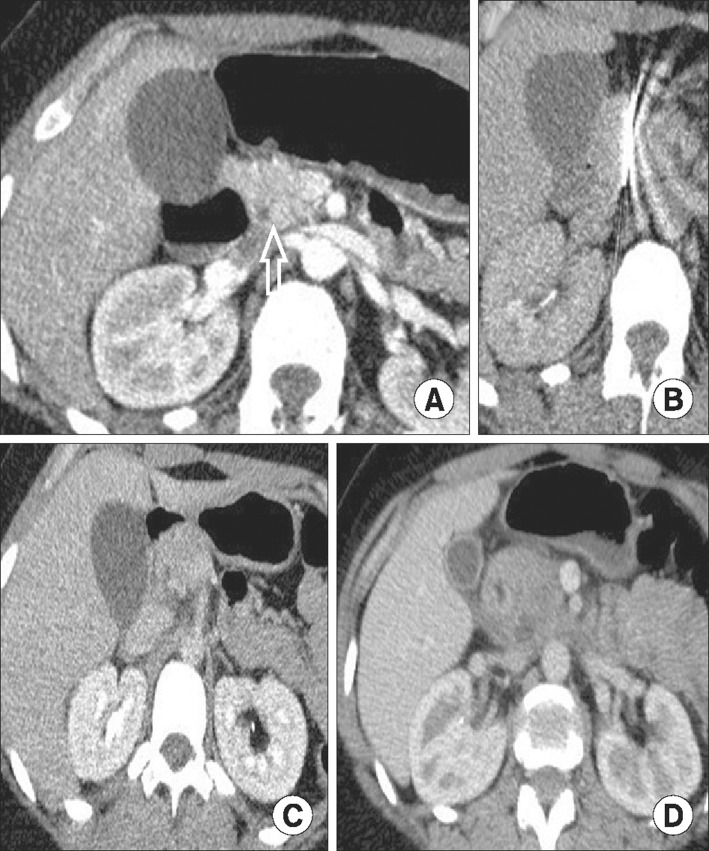 | Fig. 1Computed tomography (CT) scan showing a small hypervascular lesion at the head of the pancreas (arrow) consistent with neuroendocrine tumor (A). Irreversible electroporation (IRE) was performed using two electrodes placed percutaneously (B). CT scan 2 days post-IRE showed successful ablation (C). Three-month post-ablation CT scan showed no recurrence (D).
|
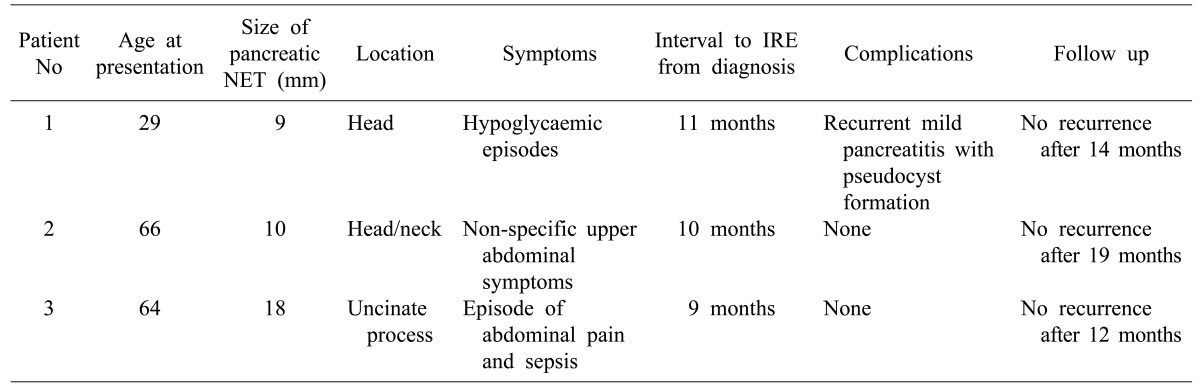
The second patient was investigated for nonspecific abdominal discomfort and indigestion and found to have a 10 mm-sized lesion with neuroendocrine features at the junction of the head and neck of the pancreas in close proximity with the SMV. Octreotide scan and biochemical neuroendocrine screen tests were both negative, but a diagnosis of pancreatic NET was corroborated by EUS findings. After a period of observation in which the tumor characteristics were unchanged, a decision was made to treat with IRE instead of pancreatoduodenectomy with possible SMV resection.
The third patient presented with an episode of abdominal pain and biliary sepsis on background of diffuse cholangiopathy, and a history of gallstones pancreatitis. An incidental finding on CT imaging was an 18 mm-sized NET in the uncinate process of the pancreas. The diagnosis was confirmed with EUS and positron emission tomography (PET) scan. The biochemical neuroendocrine screen was negative, and the patient was managed conservatively. The size of tumor was unchanged over a period of 9 months. Cholangitis resolved with antibiotic therapy. Following further discussion, IRE was offered.
Go to :
RESULTS
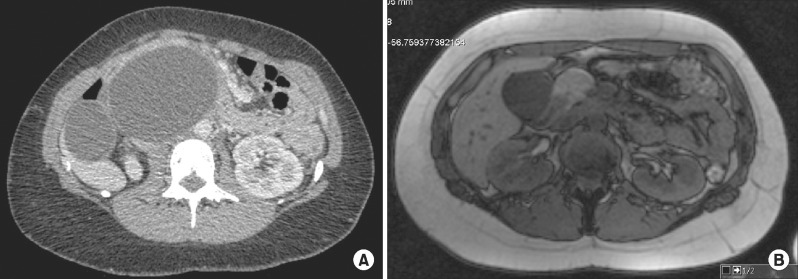
The decision to proceed to treatment with IRE was made after multidisciplinary team discussion and patient choice and approval from the New and Novel Procedure Committee from our institution was obtained. IRE (Nanoknife system, Angiodynamics, Lanthan, NY, USA) was performed percutaneously with CT guidance under general anaesthesia. There were no adverse effects during the procedure. In the first two patients, 2 electrodes were used and in the 3rd patient one additional electrode was required due to the size of tumor (Fig. 1B). Delivery of 180 pulses at 2500-3000 watts was given to each patient. Mean hospital stay was 2.6 days. The patient with insulinoma developed mild pancreatitis after procedure, which was treated conservatively. A further episode of pancreatitis was associated with a 13 cm-sized pseudocyst in the head of the pancreas. Despite the size of the cyst, the patient had limited symptoms and the fluid resolved without any intervention 4 months later (Fig. 2A and 2B). No complications were reported for the other 2 patients. Follow up at 12, 14 and 19 months with CT and MRI confirmed satisfactory ablation with no evidence of recurrence in all 3 patients (Fig. 1C and 1D). Resolution of symptoms occurred in the patient with the insulinoma, but the non-specific symptoms of the second patient did not change. The third patient continued to be monitored for cholangiopathy.
Go to :
DISCUSSION
Pancreatic NETs are a diverse group of neoplasms, with low prevalence and relatively slow progression, but strong metastatic potential. Surgical resection is currently the mainstay of treatment of the pancreatic NET even in the presence of metastatic disease. Clinical data supports the prospect of improved outcome when primary tumor is resected.1415 Small tumors (<1-2 cm) are associated with an excellent prognosis and depending on their location, enucleation rather than more radical surgery may suffice.1415 Other studies have suggested that non-functional asymptomatic tumors <10 mm may be safely observed.1617 If surgery of higher risk is considered, the option outweighs the benefit in an unfit patient. Similarly, in benign symptomatic cases (e.g., insulinoma) non-responsive to medical treatment, surgery could be avoided and ablation may be considered instead.
Ablative methods used in the pancreatic tumors, include RFA/MWA, cryoablation, photodynamic therapy, ethanol/chemotherapeutic agent injection, high Intensity focused ultrasound (HIFU) and IRE.181920 Indications include inoperable, locally advanced pancreatic adenocarcinoma and less commonly premalignant cystic and solid lesions of the pancreas.181920 EUS-guided ethanol ablation therapy for treatment of the pancreatic NETs is associated with significant co-morbidities with a 61% response rate. Improvements in ablative therapies continue and more data are required.2122 Percutaneous and endoscopic RFA has also been used, but the thermal injury associated with this technique limits its use.2324
IRE is a novel ablative technology that uses high-voltage electric pulses directed to tumor cells resulting in creation of nano-pores within the phospholipid bilayer of cell membrane, ultimately inducing apoptotic cell death.202526 It is considered superior to other ablative methods because little thermal energy is generated, underlying extracellular matrix is unaffected and adjacent vital structures such as vessels, nerves or ducts can be preserved.252627 The electrodes can be placed either percutaneously or during laparotomy/laparoscopy. Absolute contraindications include cardiac arrhythmias or implanted pacemakers/defibrillators.2728
The experience of IRE in the locally advanced, non-metastatic pancreatic cancer has shown potential benefit in locoregional palliation and overall survival, symptomatic improvement and even augmentation of the surgical margins for concomitant or subsequent curative resection.1029 Reported IRE-related complications include bleeding, bile/pancreatic leak, portal vein thrombosis, duodenal perforation (transduodenal electrode placement), pancreatitis, and cardiac arrhythmias.30 A lower complication rate was observed with the use of percutaneous IRE (9% vs. 15%). IRE–related mortality was 3% and 0% for open and percutaneous approaches, respectively. These data suggest that IRE is a relatively low-risk procedure and can safely be used in circumstances where surgery and other ablative methods are contraindicated.18293031
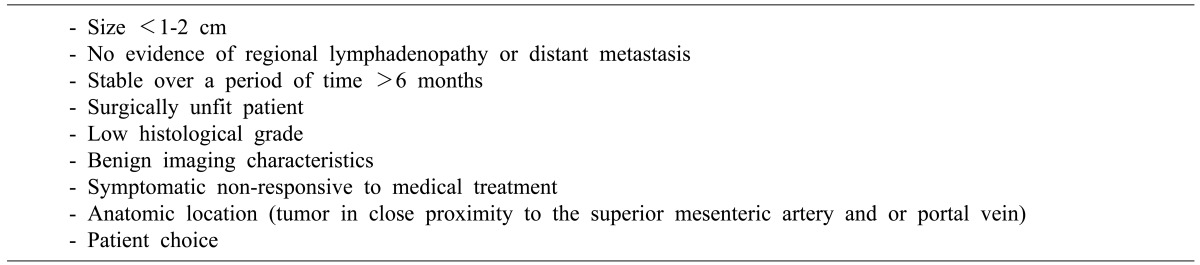
There is little available data on the use of this modality in the treatment of less aggressive pancreatic neoplasms such as NETs. This small pilot study shows that this form of locoregional therapy offers a novel approach to patients with small NETs of the pancreas or for surgically unfit patients with tumors <3 cm in diameter (Table 2).
The three cases in our study had small, low grade tumors with favorable imaging characteristics. Patients were treated following permission from the hospital novel procedures committee and informed discussion. No recurrence was observed on 12–19 months follow-up and the patient with a hormonal syndrome (insulinoma) had resolution of symptoms. Acute pancreatitis is a well-known complication of this method, and treatment does not differ from standard guidelines. In our study, the patient with the large pseudocyst was treated conservatively with significant resolution of the cyst, and is currently totally asymptomatic. The possibility of establishing a clinical trial to evaluate IRE against traditional surgical resection or enucleation deserves wider consideration.
Go to :
 XML Download
XML Download