

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The liver is the most frequent site of metastatic colorectal cancer, and metastatic lesions from colorectal cancer are frequently detected in the lungs, bones, and brain.12 As surgical managements such as operative equipment innovation, operation strategy, and perioperative management have advanced, morbidity and mortality associated with surgical resection are reduced to acceptable levels. Since the first report of liver or lung metastasectomy due to colorectal cancer,3 surgical resection of liver and lung metastatic lesions is considered the only therapeutic option for long-term survival.4 In addition, perioperative chemotherapy improves the resectability of metastasectomy with minimal safety margins, which is an accepted standard procedure that is frequently performed worldwide.5 A safety resection margin of >1 cm, or a 3-mm margin, is widely used for surgical resection of metastasis of colorectal cancer.67 Several clinical guidelines recommend surgical resection for synchronous or metachronous resectable metastatic lesions before or after systemic chemotherapy.28 However, the role of surgical resection in concomitant liver and lung metastasis is not clearly defined, and aggressive surgical resection may be a contributing factor in improvement of survival outcomes in patients with confirmed concomitant liver and lung metastasis.9 The aim of this study was to evaluate the efficacy of surgical resection in concomitant synchronous or metachronous liver and lung metastasis from colorectal cancer.
Go to : 
MATERIALS AND METHODS
Patient selection
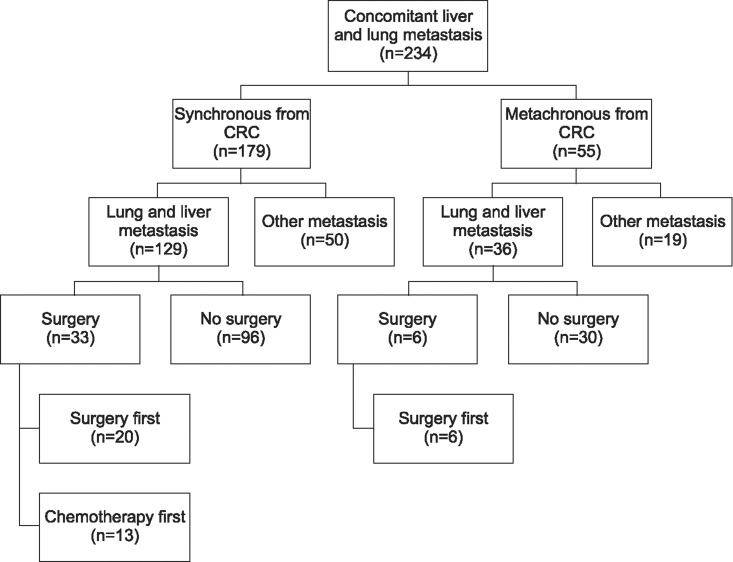
Data regarding patients with liver and lung metastasis from colorectal cancer from January 2008 to December 2012 were reviewed retrospectively in our institutional cohort. Patients with concomitant liver and lung metastasis showing solitary or multiple lesions were then selected for the study, excluding non-surgical patients and patients with other metastasis besides liver and lung. Clinicopathologic and pathologic data was obtained and survival outcomes were analyzed in these patients (Fig. 1).
Surgical procedures
Liver and lung resections were performed by hepatobiliary surgeons and thoracic surgeons at a single institution. All surgical procedures were performed to completely remove the metastatic lesions in the liver or lung. Resections of the liver and lung were conducted for solitary or multiple lesions as one-step or two-step procedure based on the surgeons' discretion.
Follow-up and survival outcome
Patients who underwent surgical resection for liver or lung metastatic lesions were examined regularly after surgery. Physical examination, blood test, and computerized tomography (CT) scan of the abdomen and thorax were performed at each evaluation. Patients were followed until the latest visiting days, including the date of death or loss to follow-up.
Statistics
Continuous variables were expressed as mean±standard deviation and categorical variables were expressed as frequencies with percentages. The Mann-Whitney U test for continuous variables and the Chi-square test for categorical variables were used to determine significant associations between parameters. The Kaplan-Meier method and log-rank test were used for survival analysis. Multivariate analysis using Cox-regression was done to identify significant prognostic factors for overall survival. Statistical significance was determined if the p-value was <0.05.
Go to :
RESULT
Patient characteristics
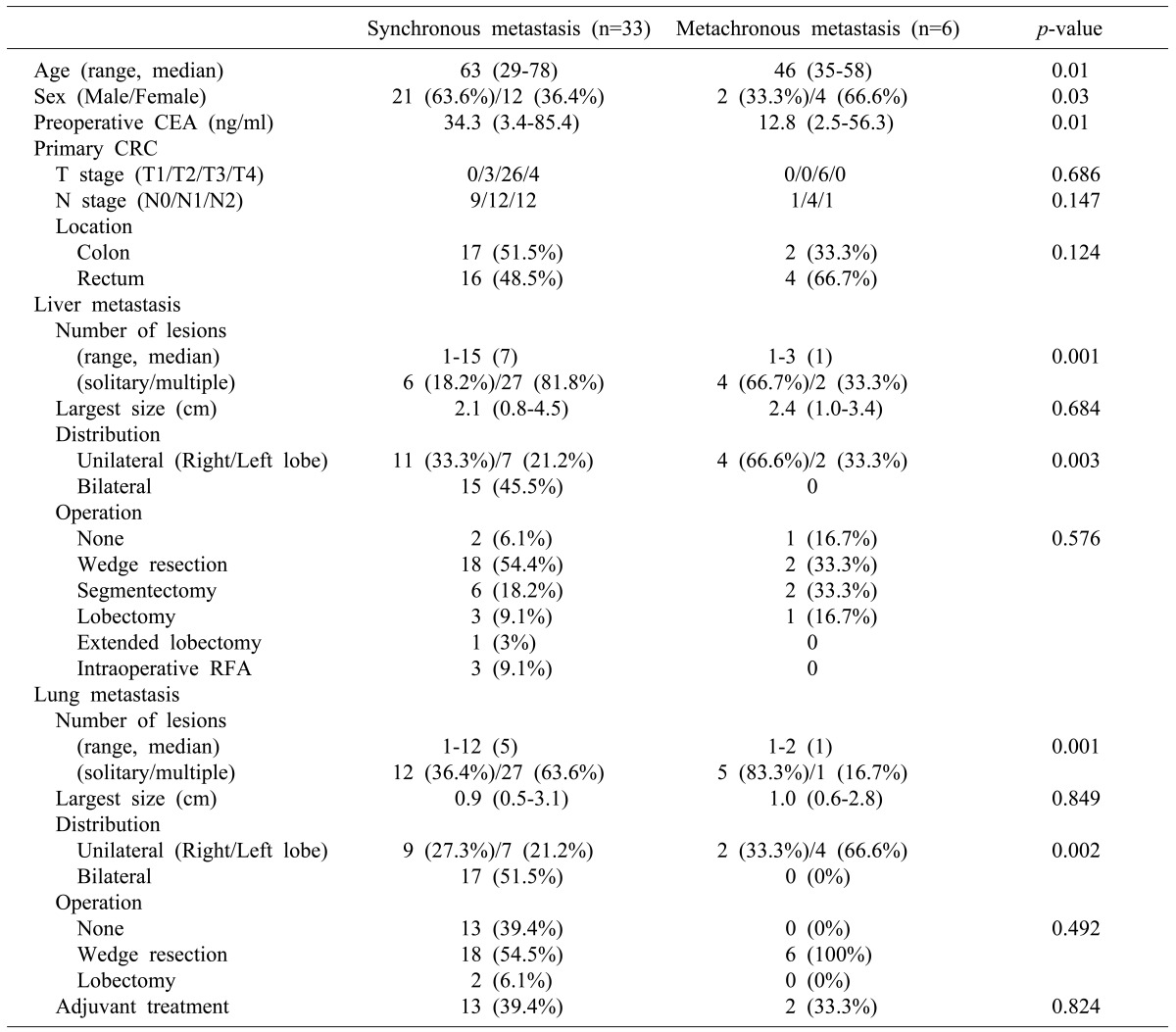
The age of patients with synchronous metastasis was significantly higher than that of patients with metachronous metastasis, and female patients were frequently identified with metachronous metastasis. T stage, N stage, and location of primary colorectal cancer was not significantly different between synchronous and metachronous metastasis patients (Table 1).
Detailed pattern of metastasis
There were more liver lesions in synchronous than metachronous metastasis, without significant difference in largest size of solitary or multiple metastatic lesions between the two groups. In addition, synchronous metastasis showed multiple metastatic lesions in both liver lobes compared to metachronous metastasis, and the surgical method was not remarkably different between the two groups.
Multiple metastatic lesions of lung in the synchronous metastases were more frequent than in the metachronous metastasis, though size of lung metastases were not significantly different for either groups. Bilateral lung metastasis was more frequent in synchronous metastasis compared to metachronous metastasis, and the surgical method was not statistically different between both groups (Table 1).
Clinical and oncologic outcomes
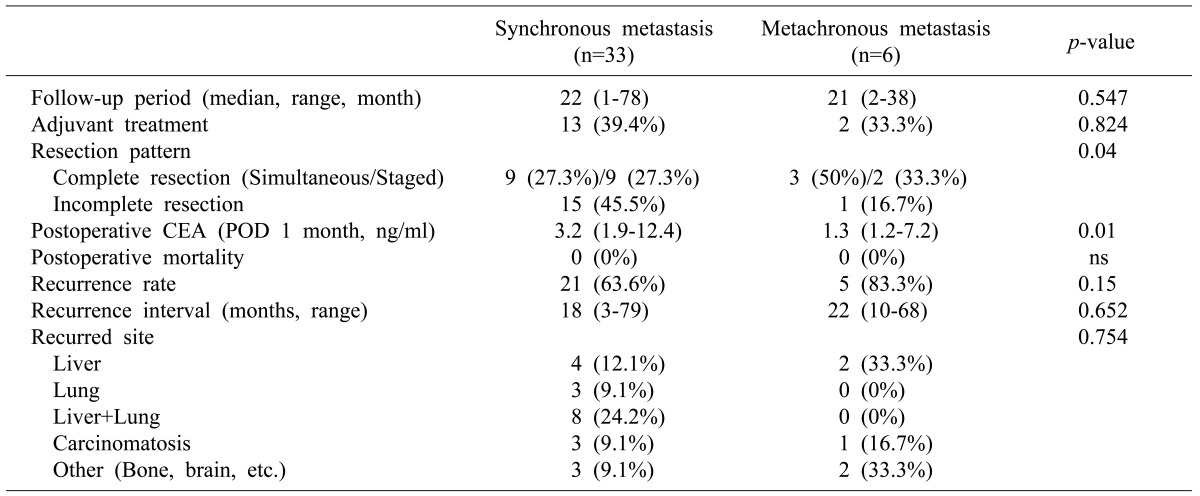
The median follow-up periods for synchronous and metachronous metastasis were 22.2 and 21.6 months, respectively, from the time of the operation. Preoperative adjuvant treatments were performed for 39.4% and 33.3% of patients in synchronous and metachronous groups, respectively. Complete surgical resections confirmed by postoperative imaging study were conducted for 54.6% and 83.3% of patients in each group. Unresected metastatic lesions in liver were treated by radiofrequency ablation (RFA) (Table 1).
There was no postoperative mortality within 30 days after operation (Table 2). Recurrence after surgical resection was 63.6% and 83.3% in the synchronous and metachronous groups, respectively. Survival analysis was performed using the Kaplan-Meier method and log-rank test. In the synchronous metastasis group, the resection group had statistically better survival, as compared to the non-resection group (p<0.001). Furthermore, complete resection of both liver and lung metastasis had significantly better survival than the incomplete resection group (p=0.037). Additionally, in the metachronous group, the resection group had significantly better survival, as compared to the non-resection group (p=0.028) (Fig. 2).
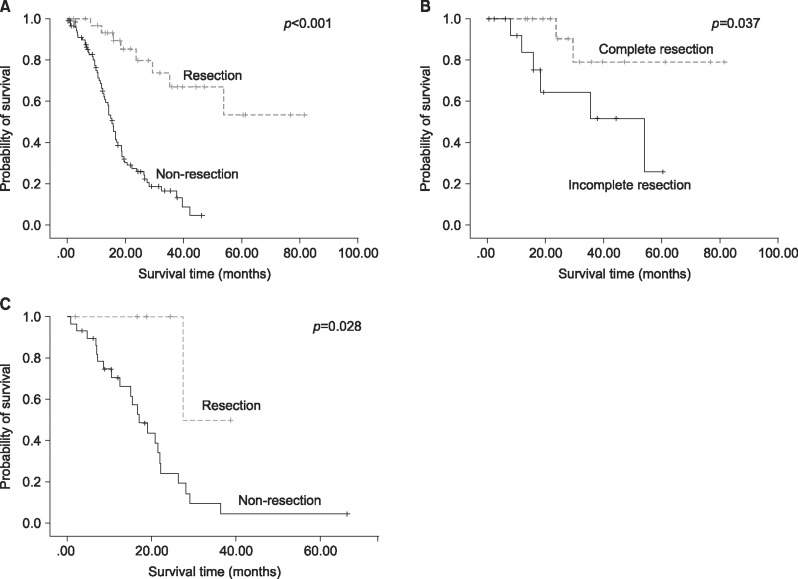 | Fig. 2Survival analysis for synchronous and metachronous metastasis from colorectal cancer. Survival analysis using the Kaplan-Meier method and log-rank test (A) in the synchronous metastasis group, the resection group showed significantly better survival compared to the non-resection group. (B) Complete resection for both liver and lung metastasis had significantly better survival compared to the incomplete resection group. (C) In the metachronous group, the resection group showed significantly better survival compared to the non-resection group.
|
Prognostic factors
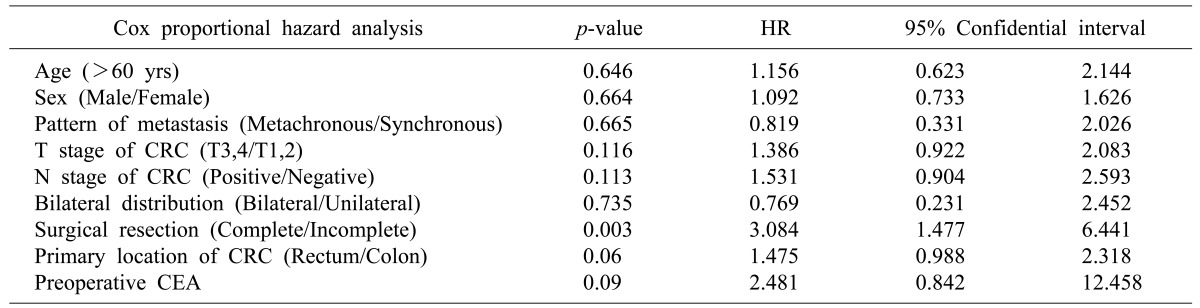
Multivariate analysis for prognostic factors of overall survival was performed using previously known prognostic factors and potential clinical markers. Rectal primary cancer was marginally significant (p=0.06, hazard ratio (HR)=0.988-2.318), and incomplete surgical resection for metastatic lesions was most significant (p=0.003, HR=1.477-6.441) for predicting poor outcomes in concomitant liver and lung metastasis from colorectal cancer (Table 3).
Go to :
DISCUSSION
Colorectal cancer leads to metastatic disease in 60% of cases, with frequent involvement of the liver, lungs, or both.5 Following several reports of promising results after surgical resection of liver metastasis from colorectal cancer, the paradigm has shifted from limited indication for hepatic resection to an active surgical approach.14 Currently, the only absolute contraindication is the inability to obtain a tumor-free margin and maintain adequate liver function. Surgical resection is the only way to achieve long-term survival in patients with colorectal cancer liver metastases;10 and several comparative studies have revealed that surgical resection shows better survival outcomes, as compared to systemic chemotherapy alone.111213
Although several studies have explored optimal treatment strategies, there are still limitations for specific guidelines in a patient with synchronous or metachronous concomitant liver and lung metastasis from colorectal cancer.910 Treatment strategy differs between institutions due to differing clinical situations of patients and the institute's management plan. Nevertheless, several studies emphasize the importance of complete surgical resection in patients with concomitant liver and lung metastasis with colorectal cancer.141516 In this study, the pattern of clinicopathologic factors, particularly the preoperative and postoperative levels of carcinoembryonic antigen (CEA), were evaluated for synchronous or metachronous metastasis from primary colorectal cancer. Although several clinical features differed based on the timing of metastasis from primary colorectal cancer, only complete resection of the metastatic liver and lung lesions improved survival outcomes.
The prognostic factors for liver and lung metastasis from colorectal cancer in terms of CEA, rectal primary cancer, bilateral lung metastasis, and multiple metastases have been recently reported.141718 In particular, complete surgical resection of both liver and lung metastasis is the most significant prognostic factor for patients with concomitant liver and lung metastasis with colorectal cancer, according to a study on the synchronism of liver and lung metastasis.9 The resectability of liver and lung metastasis has gradually increased due to the progress in surgical skill and technique, and improvement of perioperative management. Recent advances in molecular biology have also offered new prognostic factors, e.g., KRAS, BRAF, NRAS, and PIK3CA mutations, for patients with metastatic colorectal cancer in the era of precision medicine.19
This study has several limitations in terms of retrospective design, single-center study, and small study population. The heterogeneous clinical status of the enrolled population is another limitation. However, the evidence regarding the clinical situation for concurrent liver and lung metastasis in colorectal cancer is relatively rare and the strategy for this situation is not yet established. Therefore, this study increases our current understanding of concurrent liver and lung metastasis in colorectal cancer.
In conclusion, the results of this study indicated that the resection of hepatic and pulmonary metastases from colorectal cancer is safe and can offer long-term survival to selected patients. Surgery should be considered only if resection of all metastatic sites are potentially curative. Furthermore, resections should be as limited as possible to allow for repeat resections for eventual disease recurrence.
Go to :
 XML Download
XML Download