

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hepatocellular carcinoma (HCC) is the fifth most common malignancy in the world and one of the leading causes of cancer-related death.12 Liver resection is usually regarded as the preferred treatment for HCC, the downside being that it is considered as a challenging surgical procedure in the presence of liver cirrhosis.
Preoperative portal vein embolization (PVE) has long been regarded as a beneficial technique for increasing the safety of major liver resection in HCC patients through enabling volume increase in the future remnant liver (FRL). However, since a majority of HCC lesions are hypervascular, preoperative PVE carries an additional risk of rapid tumor growth from the buffering increase of the ipsilateral hepatic arterial flow. To prevent such a detrimental effect from the preoperative PVE as well as to facilitate FRL regeneration, a precedent performance of transcatheter arterial chemoembolization (TACE) is recommended before preoperative PVE for major hepatectomy.34 We previously presented that sequential TACE and PVE before surgery is a safe and effective method to increase the rate of hypertrophy of FRL and leads to longer overall and recurrence-free survival in patients with HCC.3
TACE is one of the available locoregional therapies for HCC. TACE often improves long-term outcomes in patients with unresectable HCCs, thus TACE is considered as an acceptably effective treatment for inoperable patients with large or multifocal HCCs.567 However, there were several reports supporting that preoperative TACE does not improve the post-resection prognosis - it even worsens it.67891011
Currently, most of the existing clinical studies regarding preoperative PVE with or without precedent TACE have been carried out in the form of a double-arm study with one control group of PVE only.34 The prognostic impact from TACE was primarily focused on the beneficial prevention of buffering increase of the hepatic arterial flow, but the potential detrimental effect of TACE-associated tumor spread was not taken into account. Therefore, this study was intended to shift the focus by assessing the prognostic impact of TACE before preoperative PVE on long-term survival outcomes in patients undergoing right hepatectomy for solitary HCCs through a triple-arm study comparing among the TACE-PVE group, PVE-alone group, and naïve control group.
Go to : 
MATERIALS AND METHODS
Patients
The HCC database at our institution was searched to identify patients who underwent primary liver resection for HCC in 9 years from January 2003 to December 2011, and 3582 patients were initially identified. Of them, 654 patients underwent right liver resection including right hepatectomy, extended right hepatectomy or right trisectionectomy. The detailed profiles of patients who underwent resection for solitary HCC and right liver resection were presented previously.1213
The 654 patients undergoing right liver resection were primarily screened according to the following criteria in order to avoid unnecessary bias from important prognostic factors: solitary HCC between 3.0 and 7.0 cm in diameter, right hepatectomy and extended right hepatectomy, macroscopic curative resection with tumor-free surgical margin, no macroscopic vascular invasion, no extrahepatic metastasis, no preoperative HCC treatment other than TACE within 3 months prior to PVE, hepatitis B virus (HBV)-associated background liver, and patient survival >3 months after resection. Through these screening processes, 113 patients (17.3%) were selected. Additionally, they were divided into three groups with respect to preoperative TACE and PVE as follows: the preoperative PVE group with precedent TACE (TACE-PVE group: n=27 [23.9]), the PVE-alone group (n=13 [11.5%]), and the naïve group without any preoperative preparation (control group: n=73 [64.6%]). Artificial selection of the control group patients through a propensity score-matching was not performed because these screening processes themselves worked as a strict patient selection process comparable to the usual propensity score-matching.
Medical records were reviewed retrospectively after approval by the Institutional Review Board of our institution. Patients were followed up until December 2014 through reviewing of medical records, therefore making the patient follow-up period ≥36 months or until death. All patients were completely followed up for identification of patient survival status through the assistance of the National Health Insurance Service.
Preoperative evaluation and surgical procedures
The Korean general population with chronic liver diseases have been regularly followed up for detection of HCC according to the guideline of Korean Association for the Study of the Liver.1415 Routine preoperative evaluation for HCC included abdomen and chest computed tomography (CT), magnetic resonance imaging (MRI), 2-18F-fluoro-2-deoxy-d-glucose positron emission tomography (FDG-PET) and upper gastrointestinal endoscopy. TACE was routinely performed 2-8 weeks before preoperative portal vein embolization (PVE) for major hepatectomy.16 The detailed preoperative evaluation process was presented previously.12
The extent of hepatic resection was primarily determined by the FRL volume with consideration for tumor-free resection margins and hepatic functional reserve.17
Postoperative surveillance and treatment for HCC recurrence
Patients were followed every 1 to 3 months during the first year after right liver resection, and thereafter every 3 months in principle. Most of associated patients became HBV DNA-negative during follow-up through vigorous antiviral treatment. The general principles of treatment for recurrent HCC lesions were applied to the study patients. The detailed profiles of postoperative patient follow-up were presented previously.12
Statistical analysis
The primary endpoints of this study were the overall patient survival rates after curative right liver resection. Numeric data are reported as a mean with standard deviation or as a median with range. Continuous variables were compared with the Student t-test and median test. Incidence variables were compared using the chi-square test. Survival curves were estimated by the Kaplan-Meier method and compared using the log-rank test. A p-value <0.05 was considered statistically significant. Statistical analyses were performed using SPSS (version 20, IBM, USA) and Statistica (version 6.0, StatSoft, OK, USA).
Go to :
RESULT
Patient demographics
In 113 patients of this study, most HCC lesions were detected in asymptomatic state through regular health screening or routine follow-up for liver diseases (n=94 [83.2%]). All patients were associated with HBV infection, and therefore antiviral agents were administered to 93 patients (82.3%), starting before or after surgery. During follow-up, majority of our patients showed undetectable HBV DNA and only a small proportion of patients showed very low HBV DNA titers. The baseline characteristics of the TACE-PVE, TACE-alone and control groups were quite comparable and summarized in Table 1. Mean tumor diameter was 5.1±1.7 cm in the TACE-PVE group, 4.5±1.3 cm in the PVE-alone group, and 4.7±1.2 cm in the control group (p=0.104).
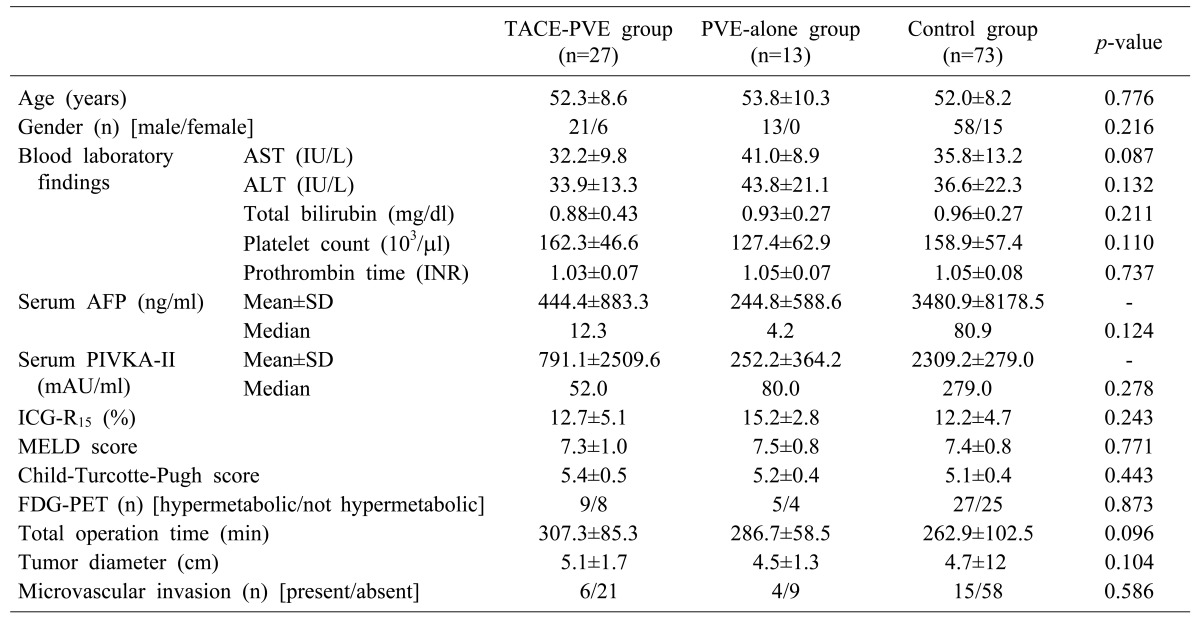
Table 1
Baseline patient characteristics of the three groups according to preoperative TACE and PVE
Continuous variables were compared with the median test and incidence variables were compared with the chi-square test between the summation of TACE-PVE and PVE-alone groups versus the control group. PVE, portal vein embolization; TACE, transcatheter arterial chemoembolization; AST, aspartate aminotransferase; ALT, alanine aminotransferase; AFP, α-fetoprotein; PIVKA-II, proteins induced by vitamin K antagonist or absence-II; ICG-R15, indocyanine green retention test at 15 minutes; MELD, model for end-stage liver disease, FDG-PET, 2-18F-fluoro-2-deoxy-d-glucose positron emission tomography
![]()
Comparison of the overall survival outcomes
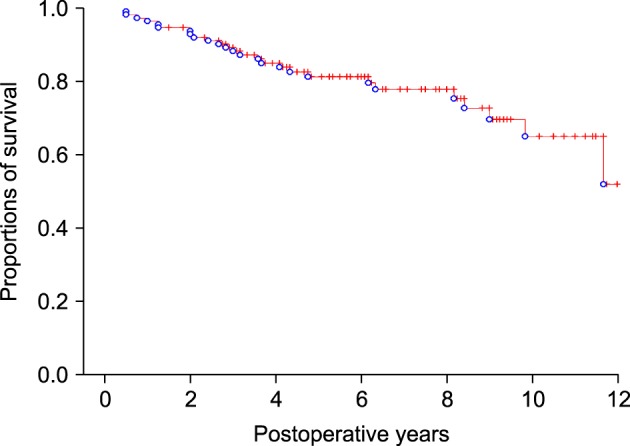
During a mean follow-up period of 70.8±39.4 months (range, 6-144) in a total of 113 patients, deaths brought about by various causes occurred in 26 patients (23.0%). The 1-, 3-, 5-, and 10-year overall patient survival rates were 96.5%, 88.2%, 81.3% and 65.0%, respectively (Fig. 1).
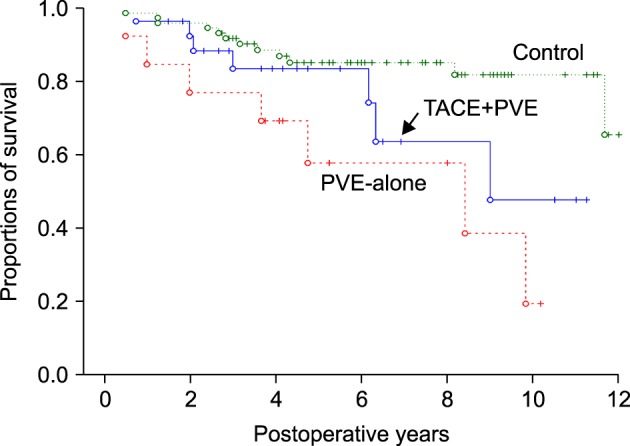
The 1-, 3-, 5-, and 10-year overall patient survival rates were 96.3%, 83.4%, 83.4% and 47.6% respectively in the TACE-PVE group; 84.6%, 76.9%, 57.7% and 19.2% respectively in the PVE-alone group; and 98.6%, 91.7%, 85.1% and 81.7% respectively in the control group (Fig. 2), showing significant prognostic deterioration in PVE-alone group (p=0.047).
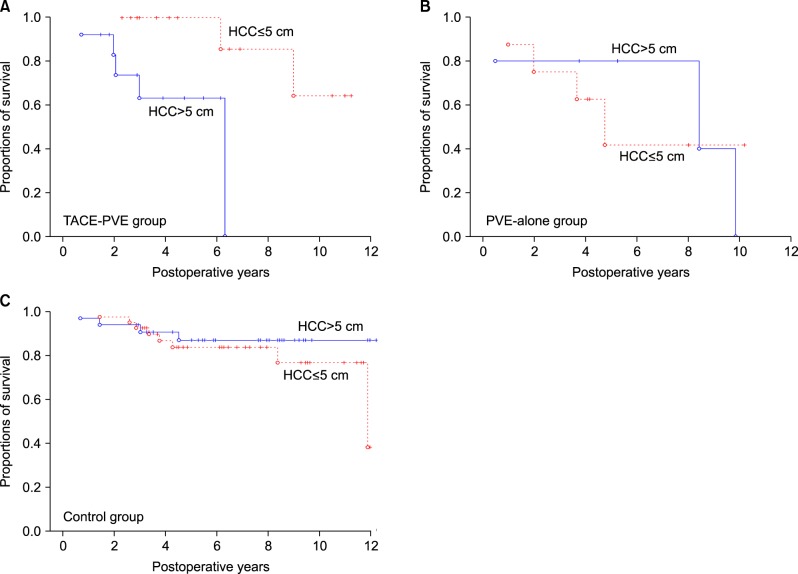
Comparison of the overall survival outcomes with a tumor size cutoff at 5 cm
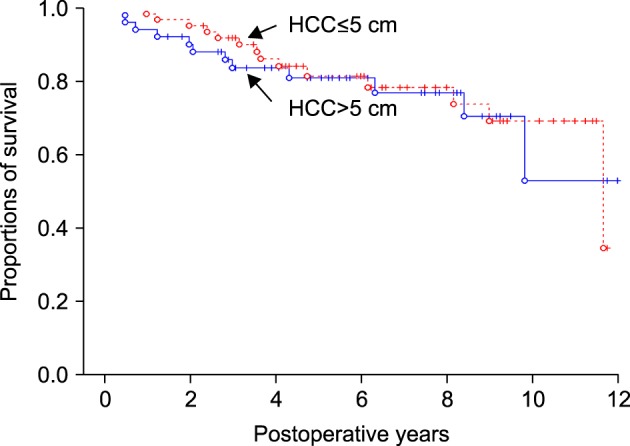
The all patients were divided into two groups by tumor size >5 cm (n=51) and ≤5 cm (n=62). The 1-, 3-, 5-, and 10-year overall patient survival rates were 94.1%, 83.7%, 81.0% and 52.9% respectively in patients with tumor size >5 cm and 98.4%, 91.9%, 81.4% and 69.1% respectively in patients with tumor size ≤5 cm (Fig. 3, p=0.774). After further division according to TACE an PVE, the tumor size cutoff at 5 cm showed significant survival difference only in the TACE-PVE group (Fig. 4A, p=0.018), but no difference in the PVE-alone group (Fig. 4B, p=0.698) and the control group (Fig. 4C, p=0.669).
Go to :
DISCUSSION
The basic concepts of sequential TACE and PVE include two aspects as follows: The first is to prevent detrimental effects from preoperative PVE, which, according to the viewpoint of surgical oncology, is the most significant challenge. The second is to facilitate further FRL regeneration. Since the interventional radiologists often emphasized the latter, there are several clinical studies supporting this concept in literature.3416 Interestingly, TACE has even been attempted even after PVE for the very purpose of FRL regeneration.16 According to these theoretical advantages, preoperative TACE-PVE may increase the probability of resectability for major hepatectomy and may decrease the risk of postoperative hepatic failure.
This study was focused on the potential prognostic effect from TACE combined with PVE. There are four randomized controlled trials that have assessed the prognostic effects of preoperative TACE so far,781819 and they similarly concluded that pretreatment with TACE alone did not improve post-resection survival. We also presented similar results after retrospective analysis.11 Due to this reason, the patient who underwent preoperative TACE alone was not included as a separate study group, thus being excluded from this study.
In the results of this study, the TACE-alone group definitely showed inferior survival outcomes than the TACE-PVE and control groups, which gives two clinical implications. The first is that PVE alone may have a negative prognostic effect. It might be associated with the potential tumor growth from PVE-associated buffering increase of the hepatic arterial flow, and subsequently it may also increase the risk of tumor cell spread.34 In contrast, it is well known that HCC tumor cell spread usually occurs through the portal venous system. We had initially presumed that PVE induces nearly complete blockage of ipsilateral hemiliver portal venous system thus transportal HCC tumor cell spread is effectively prevented, but this concept could not clearly explain the prognostic differences between the TACE-PVE and PVE alone groups. Nevertheless, preoperative performance of PVE alone would not be recommended due to inferior postoperative prognosis. The second is regarding on the working mechanism of precedent TACE to offset the detrimental effects from TACE alone and PVE alone. It might be associated with several factors. First, given that the combined treatment may induce higher tumor necrosis, there would be a lower chance of incomplete tumor resection or tumor cell dissemination during surgery34 TACE alone induces complete tumor necrosis in approximately 50% of patients.202122 It was presented that sequential TACE and PVE achieved complete tumor necrosis in more than 80% of their patients compared with only 5% after PVE alone.4 Second, the combined treatment with TACE and PVE may decrease the rate of early recurrence, which usually develops due to undetected or residual microscopic tumor after resection.23 Currently, we presume that the cytoreductive effect from precedent TACE may offset the risk of PVE-induced tumor growth, thus it may be reasonable to perform TACE before preoperative PVE. Therefore, TACE is highly recommended before preoperative PVE for major hepatectomy.
It is generally accepted that there is no size limit that precludes liver resection especially for solitary HCCs if these tumors are resectable.1224 However, the size of HCC tumors has been traditionally considered as one of the most important risk factors for tumor recurrence and overall survival. However, the concept was modified after a multi-center study demonstrated that survival outcomes were independent of tumor size in patients who underwent resection of solitary HCC without microvascular invasion.1225 In a meta-analysis of prognostic indicators in HCC treatment, tumor size was one of the most significant risk factors in 57% of good-quality studies.26 Therefore, these studies overruled the previous modification on the insignificance of tumor size on survival outcomes. We also presented that independent prognostic factors for resection of solitary HCCs were non-anatomical resection, tumor size >5 cm and microvascular invasion for tumor recurrence, and hypermetabolic uptake on FDG-PET, non-anatomical resection, tumor size >5 cm and microvascular invasion for overall patient survival.12
In this study, our patients were divided by a tumor size cutoff at 5 cm. The prognostic impact from HCC size was not overt in the PVE alone and control groups, but evident only in the TACE-PVE group. It is difficult to explain this finding clearly, but we presume that the degree of TACE-induced tumor necrosis in larger tumors would be different comparing with the smaller tumors.2728 We presented that complete necrosis after repeat TACE for post-resection intrahepatic recurrence was attained more commonly in patients with smaller tumor size and lower tumor number at first TACE and favored longer survival in recurrent patients.28 Thus, we presume that the TACE response would be reflected at the prognostic difference in the TACE-PVE group. From the oncological viewpoint of TACE response, partial tumor necrosis induced by preoperative TACE increases the risk of tumor recurrence after resection, which may be because of tumor cell dislodgement into the bloodstream.2029 The extent of tumor vascularization is significantly associated with the degree of TACE efficacy, and a high degree of vascularization is thus considered to be a predictive sign for response to TACE.3031 Thus preoperative TACE may be permissible only in HCC patients with a high degree of tumor vascularity.32 In contrast, if incomplete tumor necrosis happens, the remaining viable tumor cells are less firmly attached, and thus are more likely to be dislodged into the bloodstream before surgery and to promote the hematogenous spread of residual tumor cells during LR,1129 thus suggesting that preoperative TACE should be avoided when incomplete tumor necrosis is anticipated. We think HCC vascularity would be considered before performing preoperative sequential TACE-PVE.
The present study has several limitations. First, it is a retrospective study, thus it might be involved with some inherent flaws. Second, the sample size of the PVE groups was not large enough, thus it were not balanced with that of the control group. A uniquely strong point of this study is that the survival status of all patients was completely followed up. A prospective and randomized control trial will be required to reach definite conclusions regarding the clinical efficacy of sequential TACE and PVE before surgery.
In conclusion, preoperative sequential TACE and PVE appear to be compliant to the conventional oncological concept in addition to induction of the FRL liver regeneration. Therefore, we suggest that preoperative TACE should be come first whenever preoperative PVE for major hepatectomy is planned, especially in patients with hypervascular HCC tumors.
Go to :
 XML Download
XML Download