

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Polycystic liver disease (PCLD) is characterized by a large number of liver cysts scattered throughout the liver parenchyma. This disease entity is usually associated with autosomal dominant polycystic kidney disease. Patients with autosomal dominant polycystic kidney disease have polycystic kidneys, a feature that is absent in patients with autosomal dominant PCLD.1 Symptoms are often absent in patients with PCLD until there is a significant increase in cyst size. They mainly include abdominal pain, early satiety, dyspnea, nausea, and vomiting.2
Treatment is indicated if the symptom becomes severe or intolerable, and the therapeutic intention is to decrease the total liver volume leading to relief of compression-related symptoms.34 Most of the PCLD patients present with only disturbing symptoms that deteriorate health quality and limit daily activities rather than causing serious liver function-related complications.
There are several therapeutic options, including aspiration-sclerotherapy, cyst fenestration, partial liver resection, and liver transplantation. The choice of treatment usually depends on the number, size, and location of the liver cysts.5 The technique of fenestration of liver cysts was first described in 1968,6 which was reported to be a safe and effective treatment for the management of symptomatic non-parasitic cysts of the liver.7 In this study, we intend to present the beneficial effect of palliative fenestration treatment on quality of life in a patient with symptomatic PCLD.
Go to : 
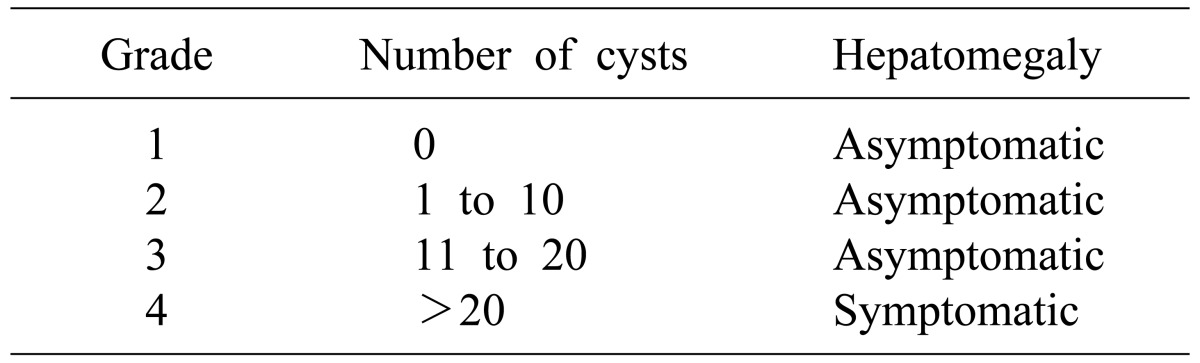
CASE
A 48-year-old female patient had been followed up for 5 years for both polycystic liver and kidney diseases at other institution. She was referred to us for identification of effective treatment. At the first visit, she complained of progressive distension of the abdomen and abdominal fullness leading to gradual decrease in body weight without shortness of breath. Her liver function was quite normal; hence, we decided to observe the patient regularly without considering palliative surgery or liver transplantation. Medical treatment with somatostatin analogue was not considered primarily due to the high medical cost as well as the undetermined therapeutic efficacy.
During the outpatient clinic follow-up for 1 year, we recognized that she had barely maintained her ability of function in daily activities due to progressive worsening of fatigue and dyspnea on exertion. Finally, she complained of shortness of breath even in a resting state. Eastern Cooperative Oncology Group (ECOG) performance status worsened from 2 to 3 during observation for 1 year.7 Gastrointestinal Quality of Life Index (GIQLI) score also deteriorated from 75 to 44 during observation for 1 year.8 Physical examination revealed that the liver was prominently bulged out of the abdomen, but leg edema was absent. Liver and kidney functions were still quite normal. Abdominal computed tomography (CT) showed progressive enlargement of multiple liver cysts with smooth and regular walls (Fig. 1), which was regarded as type III according to Gigot's classification (Fig. 2),9 grade 4 according to Qian's classification (Table 1),10 and type C according to Schnelldorfer's classification (Table 2).11 Magnetic resonance imaging study revealed water-filled multiple liver and kidney cysts (Fig. 3).
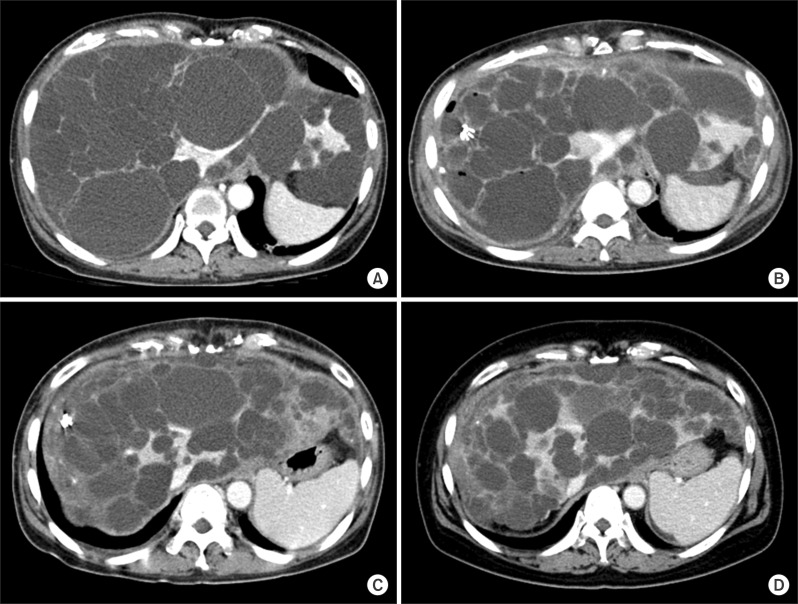
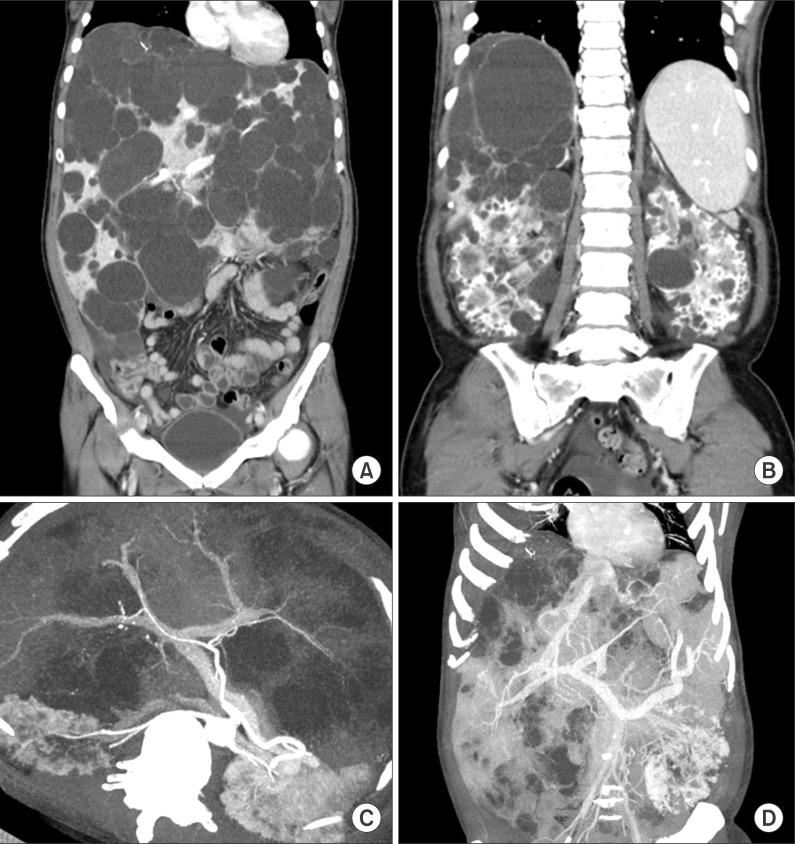 | Fig. 1Computed tomography images of the abdomen. Multiple cysts occupied the liver (A) and both kidneys (B), but the hepatic arterial and portal venous flow was well preserved (C) and hepatic veins were extrinsically compressed (D).
|
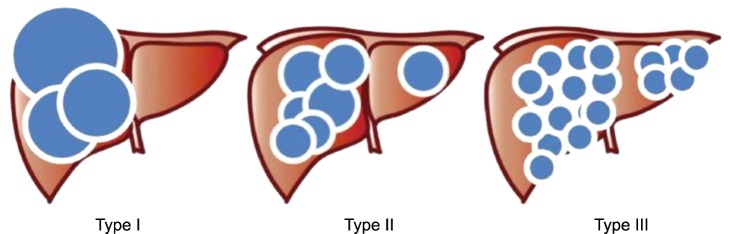 | Fig. 2Gross morphology of polycystic liver disease according to Gigot's classification. Type I: presence of less than 10 large hepatic cysts measuring more than 10 cm in maximum diameter. Type II: diffuse involvement of liver parenchyma by multiple cysts with remaining large areas of non-cystic liver parenchyma. Type III: presence of diffuse involvement of liver parenchyma by small- and medium-sized liver cysts with only a few areas of normal liver parenchyma.
|
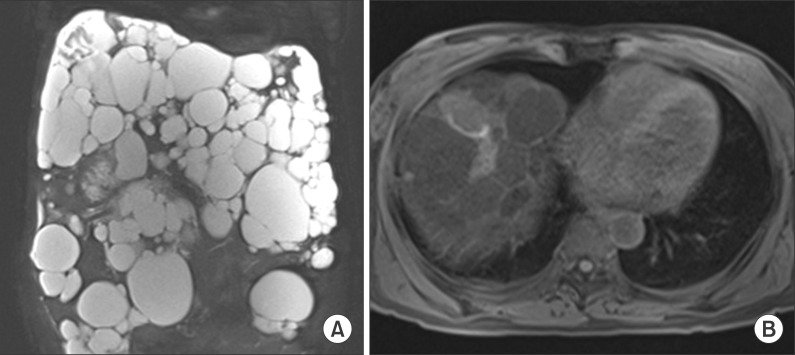 | Fig. 3Magnetic resonance imaging study of the abdomen. Waterfilled multiple liver and kidney cysts were visible (A). The gallbladder was collapsed by the adjacent liver cysts but the bile duct was not dilated (B).
|
After obtaining consent of the patient on the uncertain effect of fenestration treatment as well as high risk of disease recurrence, the patient underwent surgical fenestration treatment. Multiple cysts in the enlarged liver were opened and the cyst walls were excised with electrocautery (Fig. 4). To avoid bleeding and bile leakage, the thin membranous portions were meticulously fenestrated and none of the viable normal liver parenchyma was resected. The majority of accessible liver cysts were opened. At the end of the fenestration procedure, the liver appeared to be markedly shrunken. Three Jackson-Pratt type drains were inserted to evacuate the ascitic fluid: the abdominal drainage output was about 500 ml/day at postoperative day 1 and then it gradually decreased to less than 150 ml/day after 5 days. After performing follow-up CT at 1 week, the drains were removed. No surgical complication occurred and the patient was discharged 10 days after the open fenestration surgery. The total liver volume by using CT volumetry was 3,870 ml before surgery and 3,125 ml at 1 week after surgery, showing a volume reduction of 19.3%.
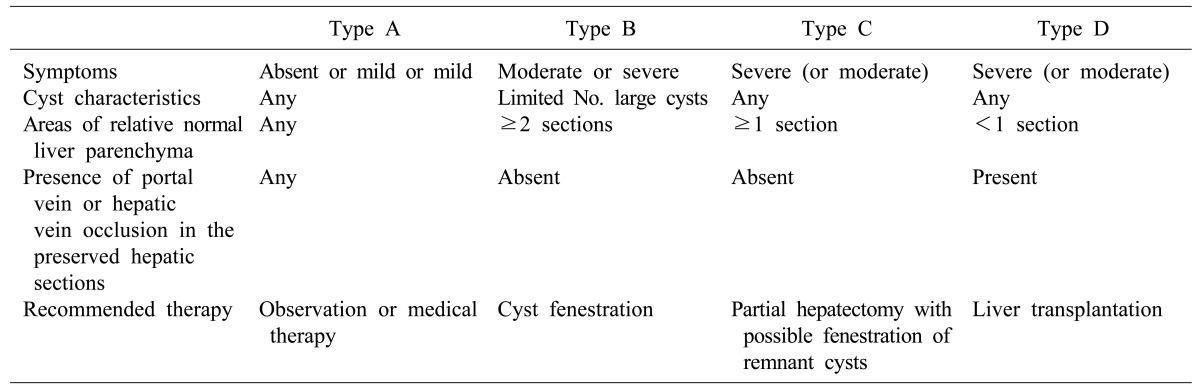
 | Fig. 4Operative findings of the patient undergoing open fenestration surgery. Enlarged liver was bulged out of the abdomen (A); There were numerous liver cysts, but the majority of liver parenchyma was preserved (B); Fenestration of the liver cyst led to moderate reduction of the whole liver volume (C); Bulging mass in the abdomen disappeared at the time of abdominal wall closure (D).
|
At 1 month after surgery, ECOG performance status improved to 1 and the GIQLI score was significantly increased to 122. During regular follow-up at an interval of 6 months, follow-up CT showed no progression in cyst size and flat abdomen was observed (Fig. 5). After 1 year, ECOG performance status improved to 0 but the GIQLI score was slightly decreased to 114. The patient is doing well and she is performing her normal activities at 18 months after surgery with no evidence of disease recurrence.
 | Fig. 5Computed tomography follow-up of the abdomen. Multiple distended cysts occupied the liver just before surgery (A); Cyst size was significantly reduced 1 week after fenestration surgery (B); No increase in the size of liver cysts was observed in the 6-month (C) and 18-month (D) images. Because of improvement in the nutritional status, subcutaneous fat was thickened in the 18-month image (D).
|
Go to :
DISCUSSION
The therapeutic intention of fenestration treatment for PCLD is to achieve relief of symptoms through liver volume reduction by rupture of liver cysts. In 1997, Gigot et al.9 evaluated 10 patients who had been treated by an aggressive attempt to reduce liver volume, mainly by open liver cyst fenestration. Deep-seated cysts were also opened with the aid of intraoperative ultrasonography, due to which the average liver volume decreased from 7,761 ml to 4,596 ml, resulting in a reduction of 43%. Both preoperative liver volume and volume reduction were greater than that obtained in the present case probably due to more extensive fenestration of deep-seated cysts. Such an aggressive approach is associated with a higher prevalence of intra- and postoperative complications such as intraoperative massive hemorrhage and a biliary tear, postoperative biliary leakage and ascites, and obstruction of the inferior vena cava. Thus, the extent of cyst fenestration should be prudently adjusted to minimize surgical complications. One study using laparoscopic fenestration showed a median liver volume reduction of 12.5%, implicating the limit of laparoscopic fenestration approach.4 Probably because high recurrence rate may be associated with low efficacy of liver volume reduction, laparoscopic fenestration for PCLD has not yet been accepted as a definitive treatment.12131415
As shown in many other studies, liver cysts are prone to becoming enlarged with the passage of time. In view of the lack of an explicit definition of recurrence, it is difficult to assess the recurrence rate after fenestration treatment in the literature.4 Some authors defined recurrence as recurrence of cysts on imaging studies, other authors defined recurrence as recurrence of symptoms, while some authors considered both symptomatic and radiological recurrence. Published series describing the results of open and laparoscopic fenestration has been summarized in the literature.16 Immediate symptom relief is achieved in 92% of the patients, whereas up to 25% experience recurrence of the cysts or symptoms.17 Complication rate after fenestration is in the range of 23% while mortality is about 2%. Factors that predict failure of fenestration are previous abdominal procedures, deep-seated cysts, incomplete unroofing, cysts in segments VII and VIII, and the presence of diffuse PCLD.17
Hepatic resection is usually reserved for highly symptomatic patients who are incapacitated by their disease due to the massive expansion of their livers.9 In such patients, fenestration alone is rarely successful because the liver parenchyma is rigid and it does not collapse.17 Symptom relief is achieved in 86% of the patients although cyst recurrence is expected in one third of the patients.18 The morbidity rate associated with this procedure can be up to 50% and includes ascites, pleural effusions, biliary leakage, and hemorrhage. One of the reasons for these complications is the fact that there is a significant distortion of the intra-hepatic vasculature and biliary tree which makes these procedures technically very challenging.
Orthotopic liver transplantation is the only curative treatment for patients with severe PCLD.19 It is indicated in those patients with disabling symptoms that lead to decreased performance status and quality of life. Patients with PCLD usually have normal liver function and the organ allocation system based on the Model for End-Stage Liver Disease (MELD) or Korean Network for Organ Sharing (KONOS) is often unable to assist this group of patients. For these patients, MELD exception criteria seem to be necessary.2021 Because of the shortage of available grafts, the need for life-long immunosuppression, and the perioperative risks, liver transplantation is indicated only in symptomatic patients (Fig. 6). In the current Korean setting in which the majority of deceased donor liver grafts are allocated to urgent patients, most patients with PCLD have a very low chance of receiving deceased donor liver grafts; therefore, some of them have undergone living donor liver transplantation.2223
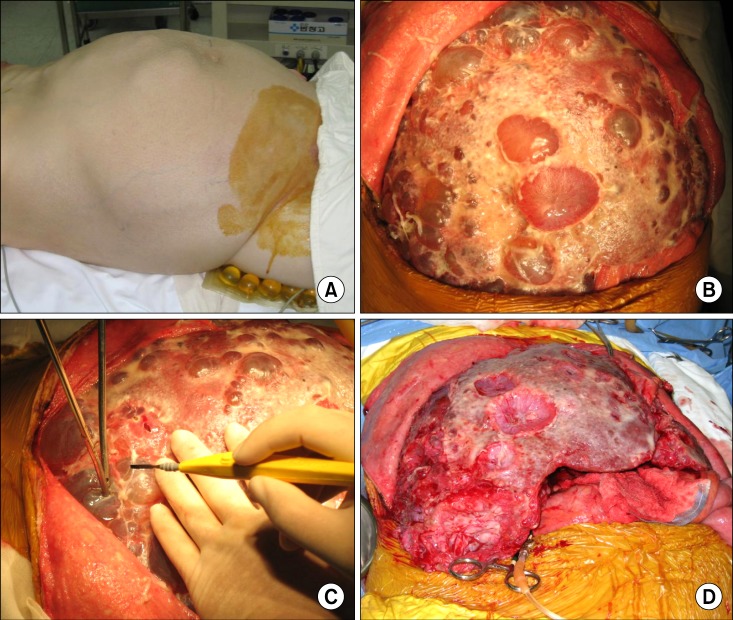 | Fig. 6Operative findings of a 52-year-old female patient undergoing liver transplantation with a MELD score of 18. Markedly enlarged liver was bulged out of the abdomen (A); There were numerous liver cysts that occupied the majority of liver parenchyma (B); Rupture of the liver cysts led to reduction of the liver volume (C), which facilitated handling of the native liver for liver transplantation (D).
|
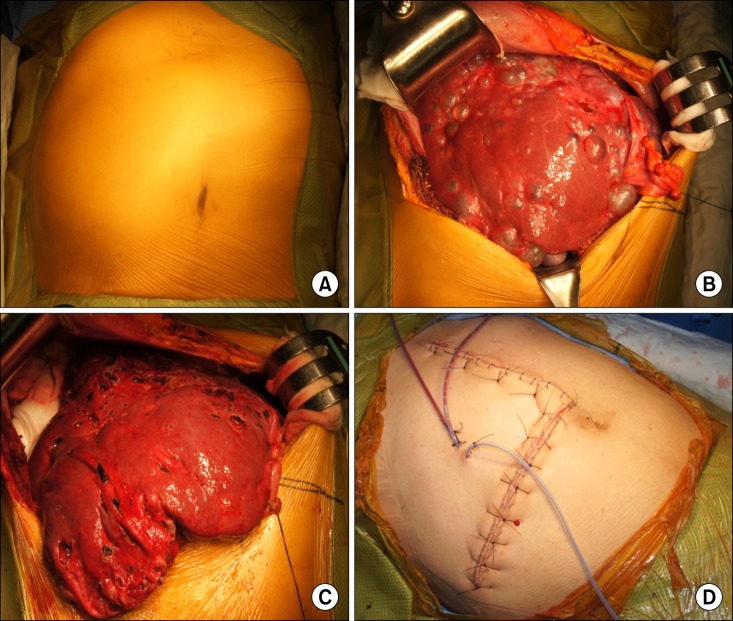
In patients with PCLD, patient selection, timing and choice of treatments can be very challenging. In symptomatic patients, treatment strategies should be based on the degree and progression of symptoms and the severity of other medical conditions. Symptomatic patients with large cysts or limited hepatic involvement might benefit from fenestration or sclerotherapy. Hepatic resection with or without fenestration should be favored in patients with diffuse involvement of the liver but with sufficiently preserved parenchyma. Finally, in the patients with diffuse disease, liver transplantation is a valid option and should be pursued as primary therapy prior to the development of debilitating disease that can significantly increase the risks of perioperative adverse events.16
In the present case, significant improvement in quality of life and daily activity performance was achieved after open fenestration treatment over 18 months of follow-up without disease recurrence.
Go to :
 XML Download
XML Download