

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hepatic portal venous gas (HPVG) is a rare radiological finding, which is associated with a poor prognosis and a mortality rate as high as 75%.12 However, with recent developments in imaging modalities, even very small amounts of gas can now be detected, which allows conservative treatment to be considered as a sufficient intervention that can be implemented early.
A surgical study of 22 patients with HPVG identified a higher mortality rate to be associated with higher Acute Physiology and Chronic Health Evaluation (APACHE) II scores and longer length of bowel resection.3 Another study documented physiological shock and pneumatosis intestinalis (PI) to be significant predictive factors for mortality; however, this study did not differentiate outcomes based on treatment method, namely surgical versus non-surgical management.4 To date, the risk factors affecting the rate of mortality in patients with HPVG who are managed non-surgically have not been clearly evaluated. Therefore, the aim of our study was to identify these factors in non-surgical patients with HPVG.
Go to : 
MATERIALS AND METHODS
A search was conducted in the radiological databases of Daegu Fatima Hospital in South Korea of the computed tomography (CT) reports of patients over the age of 18 years who had undergone abdominal CT scan. The following key words were used to identify cases of HPVG: hepatic portal venous gas, mesenteric venous gas, air portogram, PI, portal vein air. Of a total of 41941 patients who underwent abdominal CT from January 2008 to December 2014, 37 patients with the above key words were identified. Of these, 19 cases were excluded as CT scans showed only a PI without HPVG. A retrospective review of the medical records of the 18 remaining cases was performed, including a review of their CT scans by two radiology specialists to screen for the associated main portal venous gas (PVG), superior mesenteric vein (SMV) gas, PI, and other intra-abdominal pathology.
As part of the retrospective review of medical records, patients' early symptoms and underlying diseases and comorbidities were identified. Clinical condition was determined from the physical signs obtained during each patient's visit to the emergency department including the following: blood pressure, pulse rate, respiration rate, body temperature, level of consciousness, and degree of motor response to pain. The physical status for each patient was determined based on the classification system of the American Society of Anesthesiologists (ASA). The severity of each patient's status and expected risk of mortality were investigated by calculating the Acute Physiology and Chronic Health Evaluation (APACHE) II score.
For patients who underwent surgery, the worst laboratory test results obtained on the day of admission were selected for analysis. Similarly, for patients who did not undergo surgery, the worst laboratory test results obtained within 24 h after admission were used. Laboratory data included complete blood count (CBC) with differential, aspartate transaminase (AST), alanine transaminase (ALT), blood urea nitrogen (BUN), serum creatinine (SCr), electrolytes (sodium, potassium), prothrombin time (PT), partial thromboplastin time (PTT), and arterial blood gas analysis (ABGA).
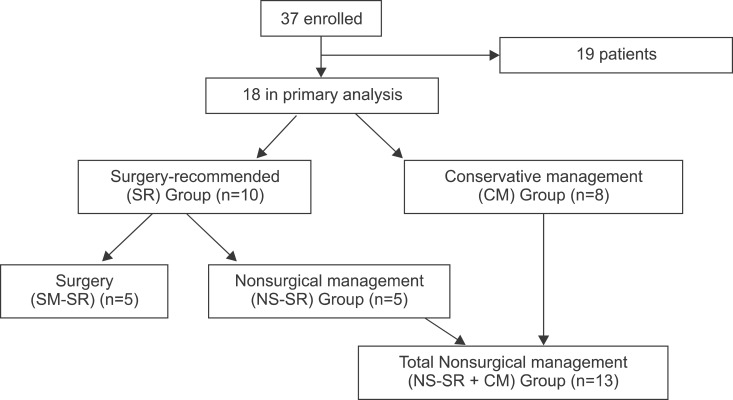
Based on the information obtained from the medical records, patients were divided into 2 groups based on clinical management status. These groups were the surgical management recommended (SR, n=10) and conservative management (CM, n=8) groups. The SR group was further subdivided into patients who underwent surgical management (SM-SR, n=5) and those who could not undergo surgery (NS-SR, n=5). Group allocation is summarized in Fig. 1.
For analysis, shock was defined as a systolic blood pressure (BP) of less than 90 mmHg despite proper hydration. Mortality was defined as death within 48 h of hospital admission. In all patients, the ASA classification, Glasgow Coma Scale (GCS) score, and APACHE II score were analyzed as prognostic factors for mortality.
Statistical analyses were performed using SPSS software (SPSS Inc., Chicago. IL, USA). Between-group differences for categorical variables were evaluated by chi-square or Fisher's exact tests, whereas between-group differences for continuous variables were evaluated by Student's t- or Welch's t-tests. For multivariate analysis, a logistic regression test was performed.
Go to :
RESULTS
The study was conducted over a 7-year period and included 18 patients. The mean age of our study group was 67.3±11.9 years, and the male to female ratio was 1:1. The distribution of gas in our study group included: 13 patients (72.2%) with PI, 10 (55.6%) with main PVG, and 8 (44.4%) with SMV gas (Fig. 2). The ileum was the most frequent site of PI (9 cases, 45%), followed by the colon (4 cases, 20%), jejunum (3 cases, 15%), cecum (3 cases, 15%), and rectum (1 case, 5%).
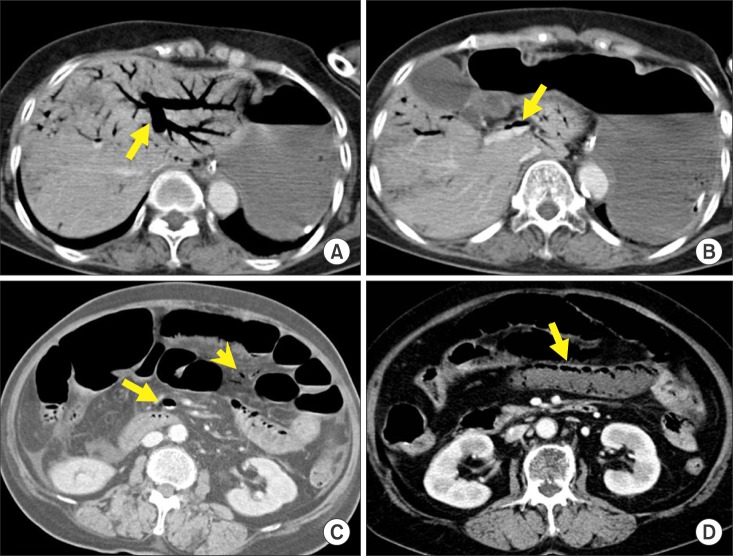 | Fig. 2Portomesenteric venous gas at different anatomical locations in various patients. Computed tomography reveals massive hepatic portal venous gas (A: arrow) and main portal venous gas (B: arrow), superior mesenteric venous gas (C: arrow), mesenteric venous branch gas (C: arrow head), and pneumatosis intestinalis (D: arrow).
|
Based on ASA physical status classification, 14 (77.8%) patients were identified as having a poor general condition (corresponding to grades III and IV on the classification scale), and the mean APACHE II score for the group was 19.9±10.3.
Disease causes and symptoms
Mesenteric ischemia accounted for 7 cases (38.9%), making it the most frequent cause of HPVG in our study group. Of these cases, 3 were caused by superior mesenteric artery (SMA) occlusion, 3 by non-occlusive mesenteric ischemia, and 1 by SMA stenosis. For the remaining patients, intestinal obstruction was identified in 4 cases (22.2%); enteritis in 4 cases (22.2%); and 1 case each of duodenal ulcer perforation (5.6%), necrotizing pancreatitis (5.6%), and diverticulitis (5.6%). The most frequently reported symptoms of HPVG were abdominal pain (83.3%), followed by nausea (61.1%), vomiting (61.1%), abdominal distension (38.9%), and diarrhea (16.7%).
Descriptive outcomes of the SM-SR group
In our study group, 10 patients were identified for whom surgical treatment was recommended based on the presence of intraperitoneal free air or bowel necrosis as confirmed by CT scan, or signs of peritoneal irritation such as rebound tenderness discovered by physical examination. However, surgery was performed in only 5 of these patients, with the other 5 unable to undergo surgery because of serious hemodynamic instability upon admission or other issues such as their caregiver's refusal to consent to surgery (Fig. 3).
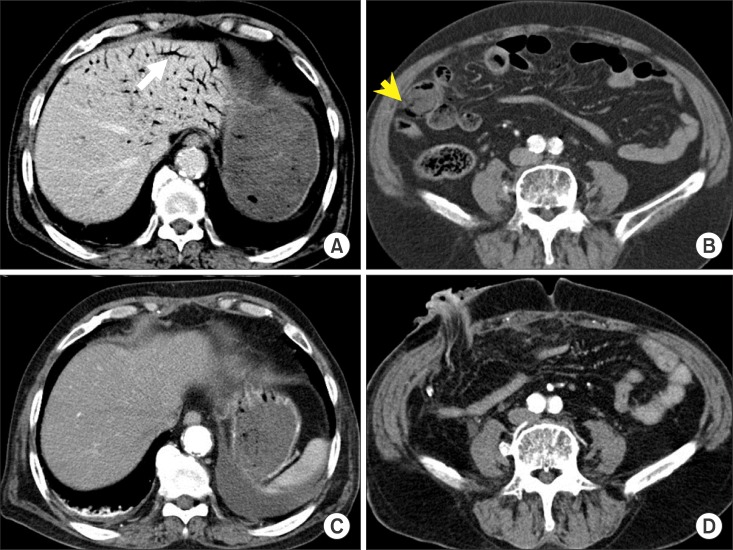 | Fig. 3A 77-year-old man with superior mesenteric artery occlusion underwent ascending colon and small bowel resection and loop ileostomy. Before operation, computed tomography demonstrates hepatic portal venous gas (A: arrow), pneumatosis intestinalis (B: arrow head). Computed tomography performed at postoperative day 12 shows absence of hepatic portal venous gas (C and D).
|
Emergency laparotomy was performed in the 5 patients in the SM-SR group. For 3 of these patients, small bowel resection (248 cm, 220 cm, and 39 cm, respectively) and end-to-end anastomosis were performed. One patient needed ileostomy and resection of the small bowel and colon (small bowel: 120 cm, colon: 38cm). The remaining patient had a duodenal perforation that required duodenal exclusion and gastrojejunostomy. Among the 5 patients who underwent surgery, 2 (40%) died on post-operative day 1. The first of these patients had alcoholic liver cirrhosis and died of disseminated intravascular coagulation (DIC), while the second patient died of acute renal failure (ARF) and adult respiratory distress syndrome (ARDS). Complications in the 3 surviving patients included: post-operative atelectasis and wound sepsis in one patient; another patient suffered from short bowel syndrome with severe diarrhea and malnutrition; and an intra-abdominal abscess formed in the last patient.
Descriptive outcomes of the non-surgically managed patients (NS-SR and CM groups)
In our study group, 13 patients were managed non-surgically (Fig. 4). Of these patients, 5 had been recommended for surgery but were ultimately not suitable candidates for surgical laparotomy due to non-consent or hemodynamic instability. For the other 8 patients, a CM approach had been recommended (i.e., the CM group). Non-surgical management included intravenous fluid therapy, antibiotics, and L-tube decompression.
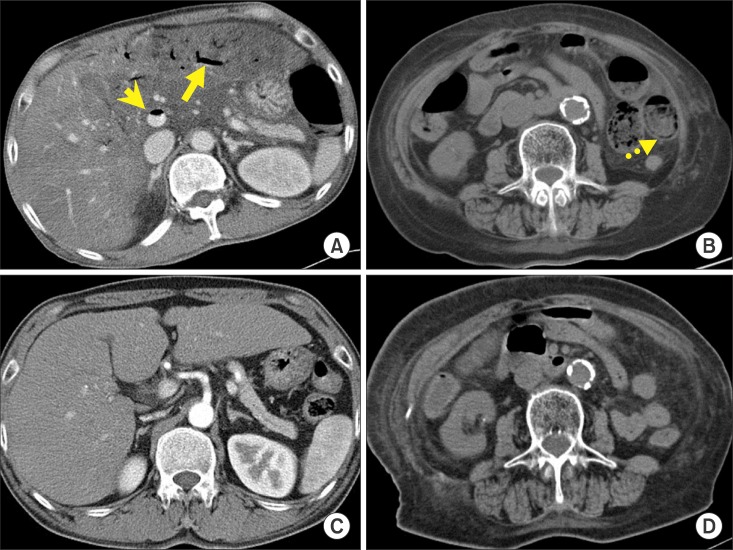 | Fig. 4An 81-year-old woman with small bowel enteritis underwent medical management. Before treatment, computed tomography shows hepatic portal venous gas (A: arrow), main portal venous gas (A: arrow head), and pneumatosis intestinalis (B: dashed arrow). Computed tomography performed at day 3 of medical treatment shows radiologic improvement (C and D).
|
Of this combined group of 13 patients managed non-surgically, 6 (46.2%) died. Of these, only 1 patient was from the CM group (mortality rate 12.5%), with the cause of death of this patient attributable to alcoholic ketoacidosis. In contrast, all patients in the NS-SR group died within 24h of diagnosis resulting in a mortality rate of 100%.
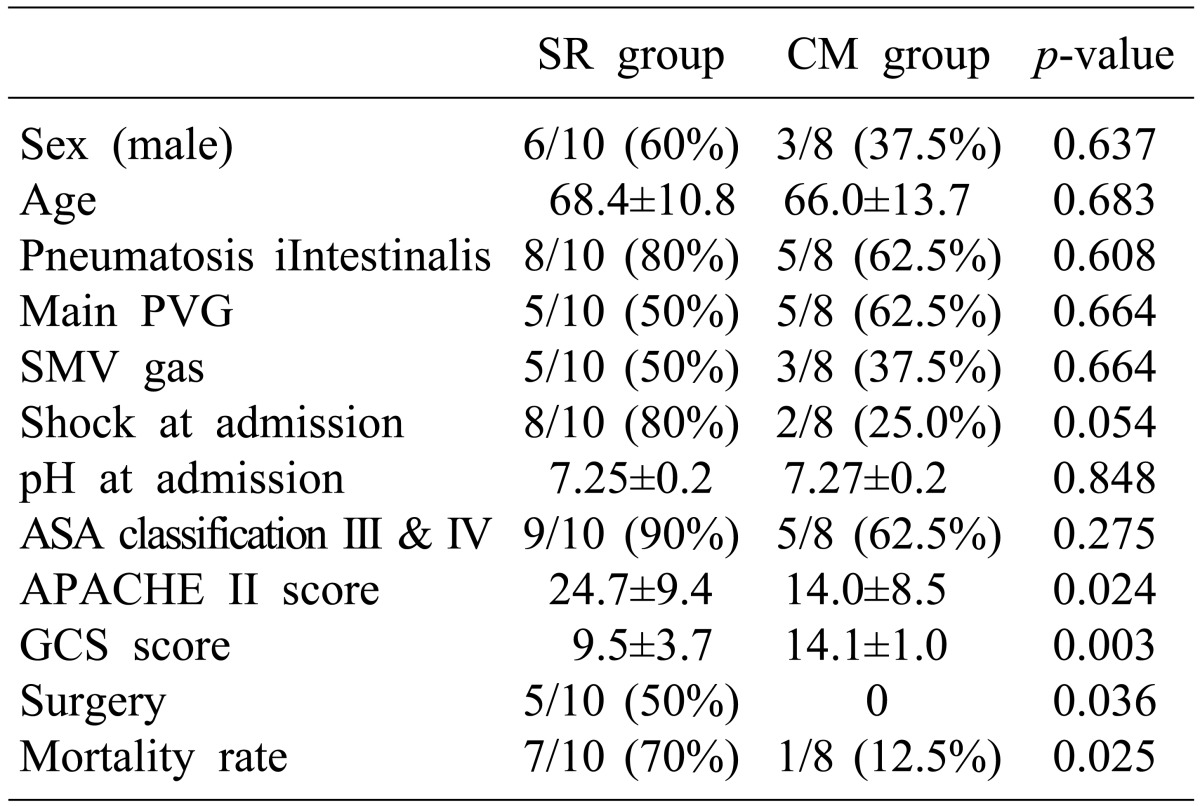
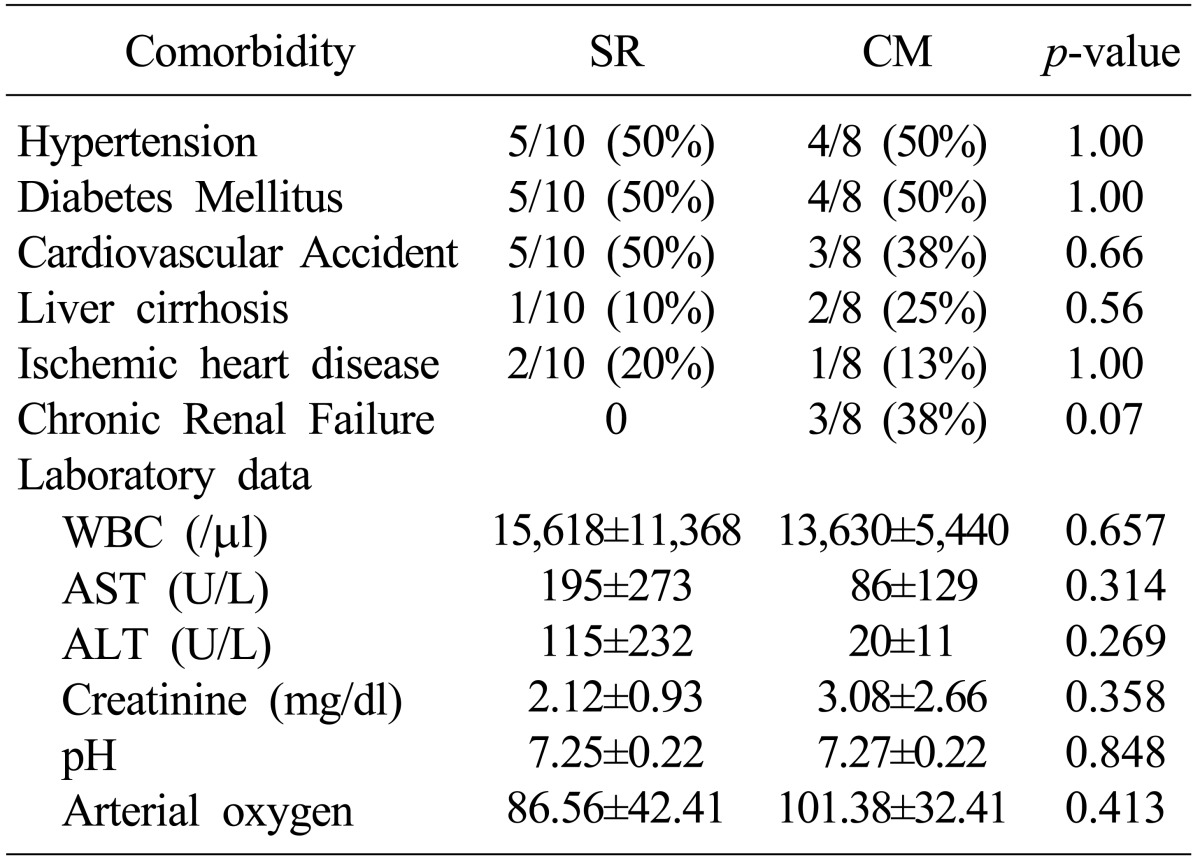
Comparison of the SR and CM groups
Both groups were comparable with regard to the male-to-female ratio; mean age; presence of PI, PVG, or SMV gas; rate and nature of comorbidities; and laboratory data. The frequency of shock and the degree of acidification at admission were higher in the SR group as compared with the CM group; however, these between-group differences were not significant. Significant between-group differences were identified for GCS score, APACHE II score, and mortality rate (Tables 1, 2).
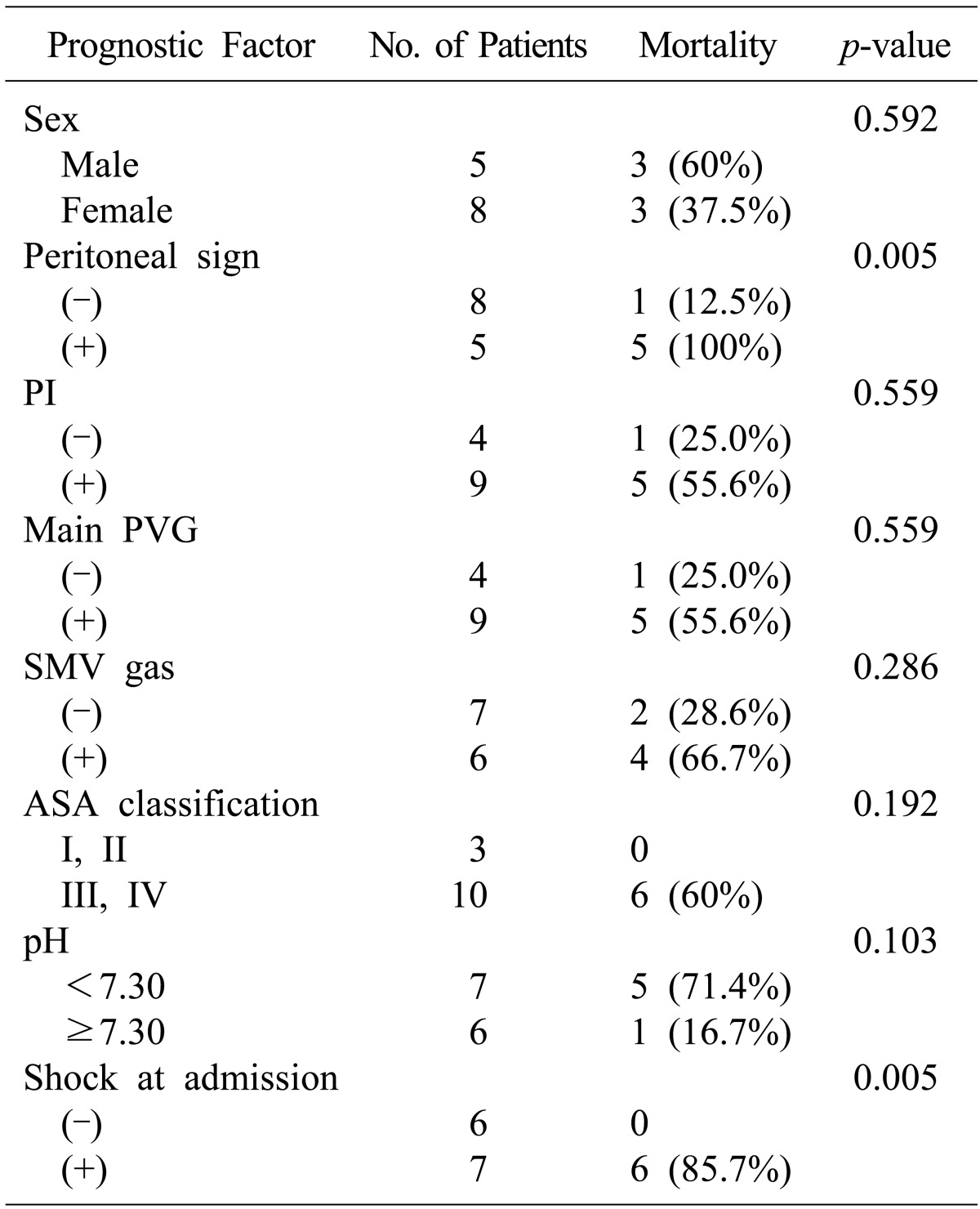
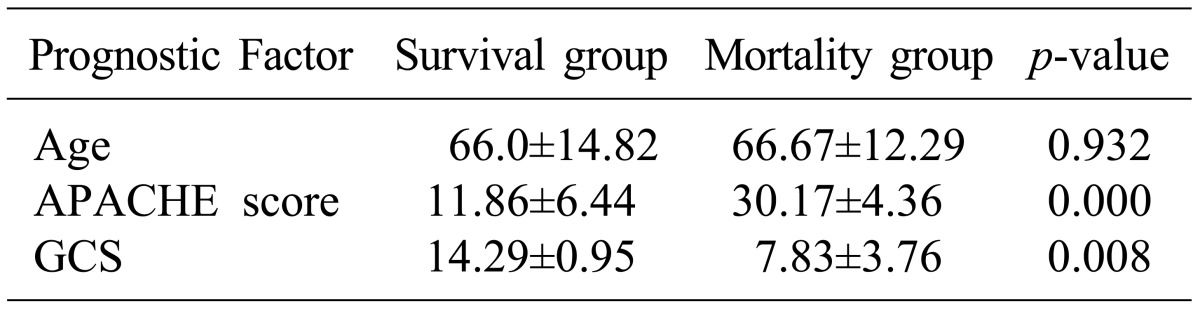
Comparison of factors affecting mortality in non-surgically managed (NS-SR and CM) groups
For the 13 patients who had HPVG and underwent non-surgical management only, the overall mortality rate was 46.2% (6/13 cases), which was relatively high. From analysis of prognostic factors affecting mortality, no difference was found between patients in the groups who survived and those who died, based on sex, age, or presence of PI, main PVG, or SMV gas. A higher but non-significant mortality rate was associated with more severe acidification at admission or with an ASA classification of III or IV. According to univariate analysis, APACHE II scores (p=0.000), GCS (p=0.008), shock at admission (p=0.005), and sign of peritoneal irritation at physical examination (p=0.005) were significant predictive variables of mortality (Tables 3, 4). Only APACHE II scoring remained a significant predictive variable in the multivariate analysis.
Go to :
DISCUSSION
Although HPVG is an ominous radiological finding, it is a non-specific sign, being associated with a range of conditions. HPVG was first reported by Wolfe and Evans in 1955, who described gas in the portal vein system of six infants who had enterocolitis.2 The clinical symptoms of HPVG include non-specific symptoms and signs such as pain, nausea, diarrhea, vomiting, abdominal distension, peritoneal irritation, and acidosis.5 The general nature of these symptoms can delay diagnosis and result in fatality when HPVG is not promptly managed.
Although the mechanism of HPVG has not been established, HPVG occurs when intestinal gas enters the vein, passing through the mucosal layer (via a damaged mucosa), due to increased pressure within the intestine resulting from increased intra-abdominal pressure.1 Another possible mechanism involves the proliferation of anaerobic bacteria within the intestine, producing a large amount of gas that enters the venous circulation.6
To identify the cause of HPVG, Kinoshita et al.7 conducted a study of 64 patients, reporting the following underlying causes of HPVG: mesenteric ischemia (43%); digestive tract dilation (12%); intraperitoneal abscess (11%); ulcerative colitis (4%); gastric ulcer (4%); complications from endoscopic procedures (4%); intraperitoneal tumor (3%); and other causes (15%). In our hospital, mesenteric ischemia was the cause in 39% of HPVG cases, a finding comparable to that of Kinoshita et al.7
HPVG can be diagnosed by radiographic examination such as through plain abdominal radiography, ultrasonography (USG), color Doppler flow imaging, or CT.8 Among these, CT is the best diagnostic method because of its high sensitivity to HPVG and its capability in concurrent investigation of underlying diseases or abdominal pathology.91011 Moreover, in critically ill patients with poor vital signs, CT can be performed quickly, with little influence of practitioner or patient factors on results. In our retrospective case series, CT was used to diagnose all the patients.
There is an ongoing debate regarding the correlation between the associated SMV, mesenteric vein gas or PI in HPVG patients and mortality rate. Heye et al.12 reported a higher mortality rate in a group of 47 patients with HPVG when gas was present in the SMV. Morris et al.13 advocated that the combination of HPVG and PI increases mortality. Another study reported that HPVG accompanied by PI increased the risk for fulminant bowel infarction.14 In contrast, Faberman and Mayo-Smith9 found no association between mesenteric vein gas and mortality. Another study reported that PI and HPVG do not reflect the severity of bowel ischemia.15 In our study, presence of PI, main PVG, and SMV gas did not affect the mortality rate, leading us to conclude that the distribution of gas in the venous system was not associated with mortality.
Until 1978, when HPVG was first detected, the mortality rate approached 75%.1 As diagnosis of HPVG was based on the conventional abdominal films available at that time, HPVG was diagnosed only when there was a large amount of gas, and therefore bowel necrosis was already present in many cases. Recently, the mortality rate associated with HPVG has decreased to between 29% and 39% as a result of improved diagnosis using CT or USG, which allows detection of even a small amount of HPVG, and improvements in treatment.71112 For all HPVG patients in our study, the mortality rate was 44.4% (8/18), a rate somewhat higher than the rate reported in previous studies. This difference in the mortality rate can be explained by the relatively large number of patients for whom surgical management was recommended but, for various reasons, underwent conservative treatment instead. The mortality rate among patients who underwent surgery for intra-peritoneal free air or bowel necrosis identified by CT was 40% (2/5, SM-SR group), a rate lower than the mortality rate for patients who received only medical treatment (46.2%, 6/13, NS-SR and CM group). Patients receiving only medical treatment included those who would not have tolerated a surgical procedure or who refused surgery.
A number of studies have evaluated the risk factors affecting mortality rate in patients with HPVG. One study reported that a high APACHE II score and longer resection of the small bowel were significantly associated with higher mortality.3 Another study reported that shock at admission and PI were significant risk factors for HPVG-related mortality.4 In our study, a high APACHE II score was identified as a predictive factor of mortality among patients receiving only medical treatment.
If HPVG can be detected early in its course by imaging modality, then what is the best course of treatment? Based on our outcomes, we postulate that the decision to proceed with surgical intervention over conservative treatment should be carefully considered, taking into account clinical symptoms, laboratory findings, and radiographic findings. Nelson et al. published an "ABC" algorithm, which stresses that operative treatment (Aggressive treatment), close monitoring (Be careful), and medical treatment (Conservative treatment) should be carried out, depending on the patient's condition.6
In conclusion, when HPVG is detected via imaging, all patients should not necessarily undergo surgery. However, in our study, among patients of the SR group who were managed non-surgically (NS-SR), all (5/5) died within 24h of diagnosis. In patients (13/18) receiving only medical treatment, a higher APACHE II score was identified as a predictive factor of mortality. Thus we propose that, if surgical indication is present, emergent laparotomy is essential, and in medically-managed patients with a higher APACHE II score, indications for surgical management should be judiciously evaluated considering that aggressive laparotomy can increase survival.
In this study, the prognostic factors affecting the mortality rate of patients with HPVG were investigated. However, our study was limited by its retrospective design and a small sample size not representative of the general characteristics of all patients with HPVG. Prospective multicenter studies targeting a larger number of patients with HPVG should be conducted in the future.
Go to :
 XML Download
XML Download