

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Pancreaticoduodenectomy (PD) is associated with high mortality and morbidity, although surgical techniques and perioperative managements can improve its outcomes. One of the major causes of morbidity after PD is the failure of healing at the pancreaticoenteric anastomosis presenting as a pancreatic fistula (PF).1234 PF is associated with other major complications such as bleeding, delayed gastric emptying, intraabdominal abscess, and wound infection. Many surgical and medical methods have been used to reduce the incidence of PF, including various technical modifications of pancreaticojejunostomy (PJ) reconstruction, wrapping with omental patch graft, use of fibrin glue sealant around the PJ, and postoperative administration of octreotide.56789101112 However, most of these methods have failed to demonstrate a substantial reduction in the occurrence of PF after PD.
Once pancreatic leak fluid is infected, it is difficult to effectively control peripancreatic abscess and drain tract infection probably due to the persistence of pancreatic leak. It becomes one of the leading causes of pseudoaneurysm formation. Thus, effective drainage method plays an important role in converting the pancreatic leak into controlled PF instead of making intraabdominal abscess formation around the PJ site.13
To cope with such troublesome situation of intractable pus drainage from persistent pancreatic leak after PD, we have empirically performed local administration of high-concentration cocktail of antibiotics into the abdominal drains. The purpose of this study was to assess its therapeutic effect in patients with intractable pus drainage after PD.
Go to : 
MATERIALS AND METHODS
Patient selection
During the study period of 6 years between January 2009 and December 2014, ten patients who underwent PD due to periampullary malignancy received local administration of high-concentration cocktail of antibiotics due to intractable pus drainage from the abdominal drains. These patients were assigned into the study group.
To perform a comparative study, we selected another 10 patients who underwent PD due to periampullary malignancy for the control group after reviewing their medical records. They were selected through propensity score matching as follows: patient demographics, primary disease (distal bile duct cancer and ampulla of Vater cancer, types of PD (pylorus-preserving PD [PPPD] only), consistency of pancreatic parenchyma (soft nature only), diameter of the pancreatic duct (<5 mm), types of pancreaticojejunal anastomosis (end-to-side type with duct-to-mucosa reconstruction), types of abdominal drainage method (multiple drain insertion including closed-suction type cigarette drain), degree of pancreatic leak (grade B and C), and culture-proved microorganisms.
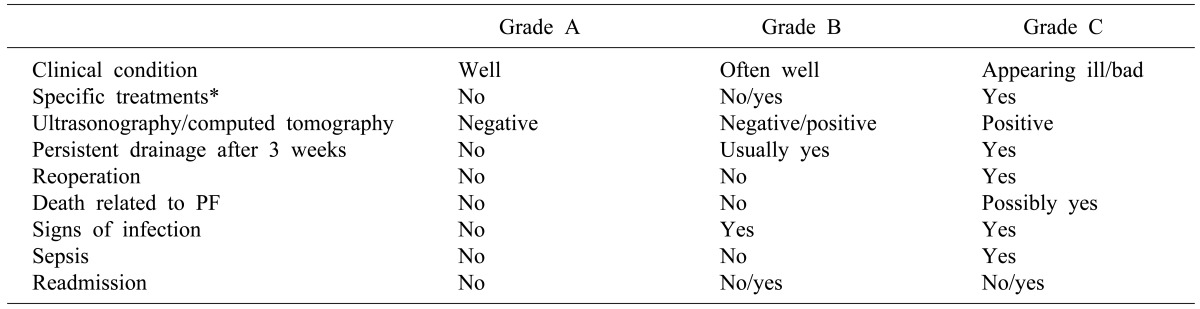
For the diagnosis of pancreatic leak, an amylase concentrations in the drain of more than three times of the serum value on day 3 or more after surgery was used to define patients with positive drain amylase. Postoperative pancreatic leakage was graded according to the classification of the International Study Group on Pancreatic Fistula (ISGPF) (Table 1).141516
Surgical procedures
All patients in both the study group and the control group underwent PPPD with internal or external pancreatic drainage. For external pancreatic drainage, a silastic external drainage tube was inserted into the pancreatic duct during PJ procedure and pulled out from the jejunal limb through a 3-cm-long Witzel tunnel. A Jackson-Pratt type drain tube of 3.2 mm in external diameter was used as an external drainage tube after cutting the distal end portion of suction slits so that the tube could be firmly inserted into the pancreatic duct of the remnant pancreas (pancreatic duct of 2.5-4 mm in diameter). If the diameter of the remnant pancreatic duct was too small for this tube (i.e., <2.5 mm), a thinner silastic tube of 2.5 mm was used in external diameter. These tubes were transfixed with 4-0 Chromic catgut suture at the pancreatic duct suture line as well as at the end of Witzel tunnel to prevent unwanted early removal.17 The external drainage tube was removed from patients 3 to 4 weeks after PPPD.
For internal drainage, a silastic tube with 5-15 cm in length was inserted into the remnant pancreatic duct and then transfixed with 6-0 Prolene during PJ procedure. The same tube was used for both external and internal drainage according to the pancreatic duct diameter. The tube was cut short for the purpose of internal drainage. For patients with remnant pancreatic duct >4 mm, internal pancreatic stent was not inserted routinely.18
Fibrin glue sealant was applied over the PJ site. The omental patch graft was also attached if possible. In addition, two or three suction-type cigarette drains around the PJ site were inserted. Multiple side-holes in a 10 mm-wide silastic Penrose drain and a 4.8 mm-sized Jackson-Pratt silastic tube were made. These two tubes were integrated as in conventional cigarette drain. The outside portion of this drain was tightly tied to prevent air leak while the inner drainage tube was connected to a Jackson-Pratt type suction bag.13
Perioperative follow-up for pancreatic leak
Multidetector dynamic abdominal computed tomography (CT) was performed at 7 days and 14 days in routine checkups. For the diagnosis of pancreatic leak, the concentrations of amylase and lipase in the drain were measured daily or every other day for more than 1 week.
Statistics
Continuous variables were reported as means±standard deviations (SD). They were compared between the two groups using independent t-tests. Incidence or categorical variables were presented as frequency distributions. They were compared between the two groups using two-tailed Fisher's exact test and chi-squared test. Statistical analyses were performed using SPSS software (version 21, IBM, USA). Statistical significance was considered when p-value was less than 0.05.
Go to :
RESULTS
Demographic and surgical profiles of patients
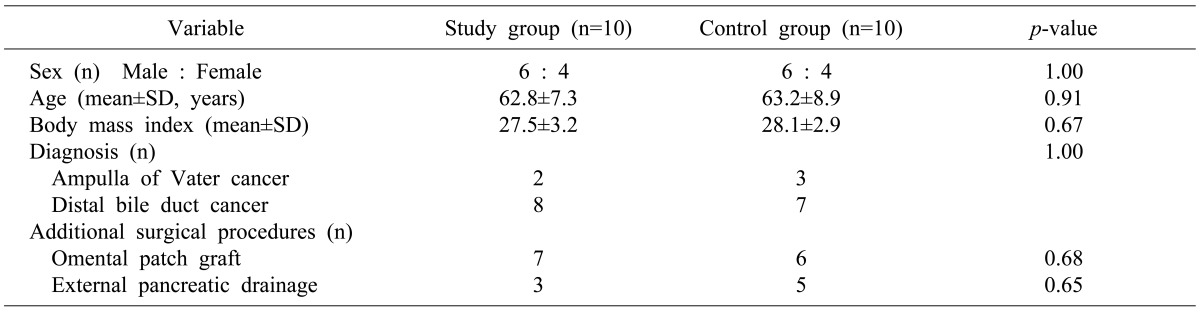
The demographic and surgical characteristics of both study and control groups are summarized in Table 2. Patient profiles and the degrees of pancreatic leak in the study group were similar to those in the control group.
Pancreatic leak and management
Postoperative PF of grade B and C occurred in 7 and 3 patients, respectively, in the study group. Grade B and C postoperative PF occurred in 9 and 1 patient, respectively, in the control group (Table 3). Patients of PF grade C were graded primarily due to septic episodes, although none of them underwent additional interventional procedure or needed repeat surgery.
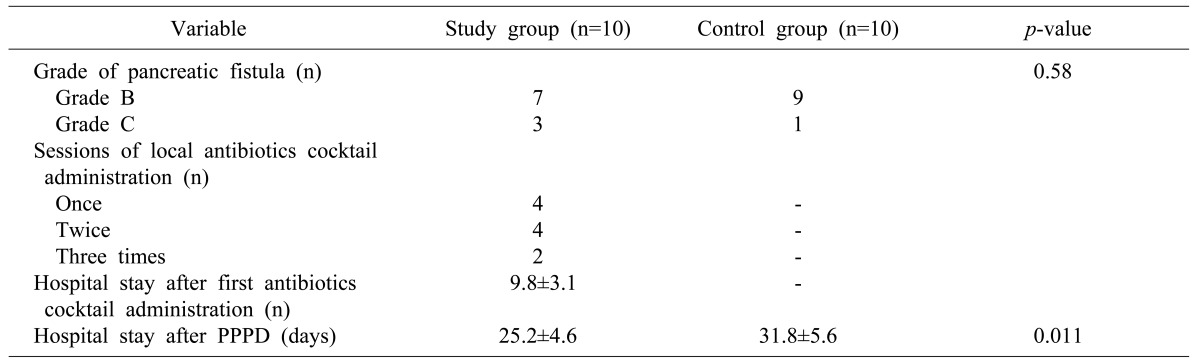
In the study group, a total of 18 sessions (mean 1.8 sessions, Table 3) of antibiotics cocktail solution was administered to the 10 patients through closed cigarette suction drains that were placed around the PJ site. Before antibiotics cocktail administration, dynamic CT was taken to assess the status of pancreatic leak and abnormal fluid collection to obtain baseline imaging information.
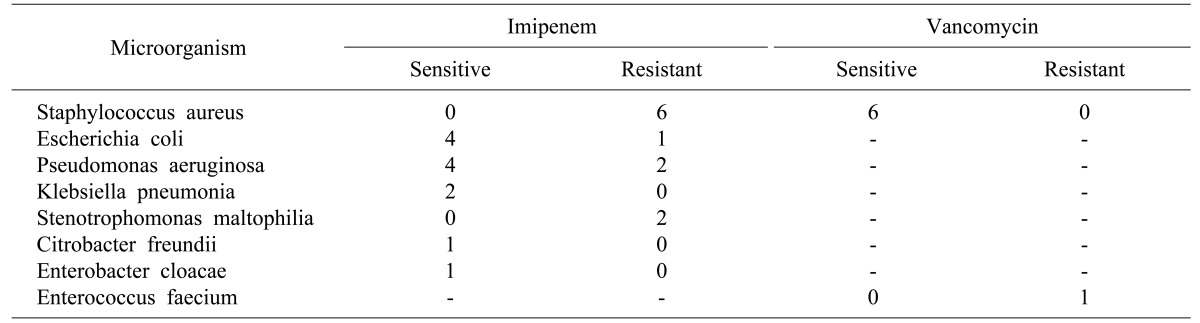
Imipenem 500 mg and vancomycin 500 mg were dissolved in 20 ml of normal saline to obtain a very high concentration solution. The two antibiotics were selected empirically or based on antibiotics sensitivity (Table 4). For two pus-draining abdominal drains, each 10 ml of antibiotics cocktail solution was injected into one drain. Suction bag was applied immediately. This procedure delivered less than 10 ml of antibiotics cocktail solution into the abdominal cavity, thus preventing wide spillage of pus and antibiotics around the drain insertion site. The antibiotics would be dispersed slowly around the injection area. This local administration of antibiotics cocktail solution was repeated one day or two days later depending on the response to the first session.
Following the first-session antibiotics administration, eight patients showed no noticeable adverse effect (Fig. 1). However, two patients showed sudden onset of febrile episodes a few hours after the local administration. Follow-up CT scan performed the next day showed no significant change in one patient. However, another patient showed increase in abnormal fluid collection due to a total of 40 ml solution was accidentally injected into the drains (Fig. 2). In these two patients, fever was spontaneously controlled within 48 hours. At 2 to 4 days after the first-session antibiotics administration, pus-like drain discharge turned to be serous with significantly decreased amount. When such response appeared suboptimal, local antibiotics administration was repeated once or twice again. In all 10 patients, abdominal drains were successfully removed within 10 days after the last session of local administration. This led to shortened postoperative hospital stay comparing to the control group (Table 3). In both study group and control group, no patient received radiological or surgical intervention due to PF-associated complications.
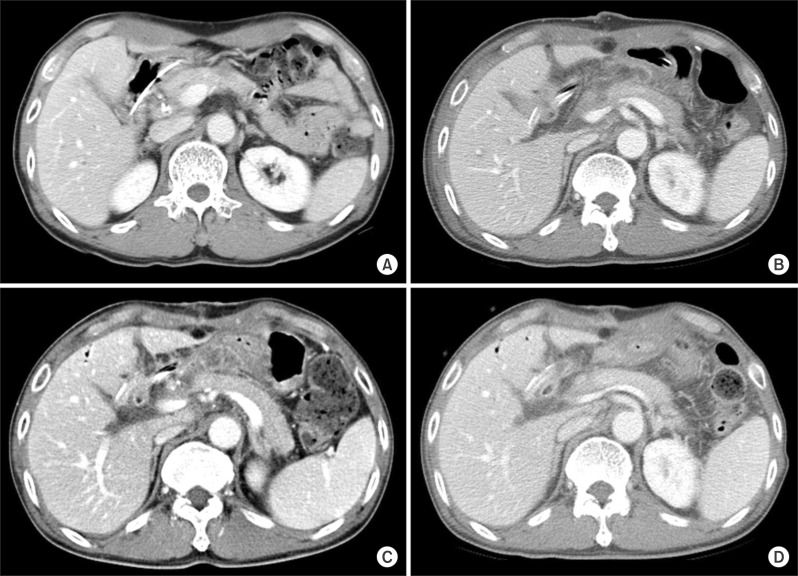 | Fig. 1Uneventful sequences of trans-drain administration of small amount of high-concentration antibiotics cocktail solution in a 63-year-old male patient with distal bile duct cancer. Computed tomography (CT) images are operative CT image (A), 1-week CT image showing abnormal fluid collection around the pancreaticojejunostomy site (B), 2-week CT image showing increase of abnormal fluid collection before trans-drain antibiotics administration (C), and 3-week CT image showing marked resolution of abnormal fluid collection 5 days after trans-drain antibiotics administration (D).
|
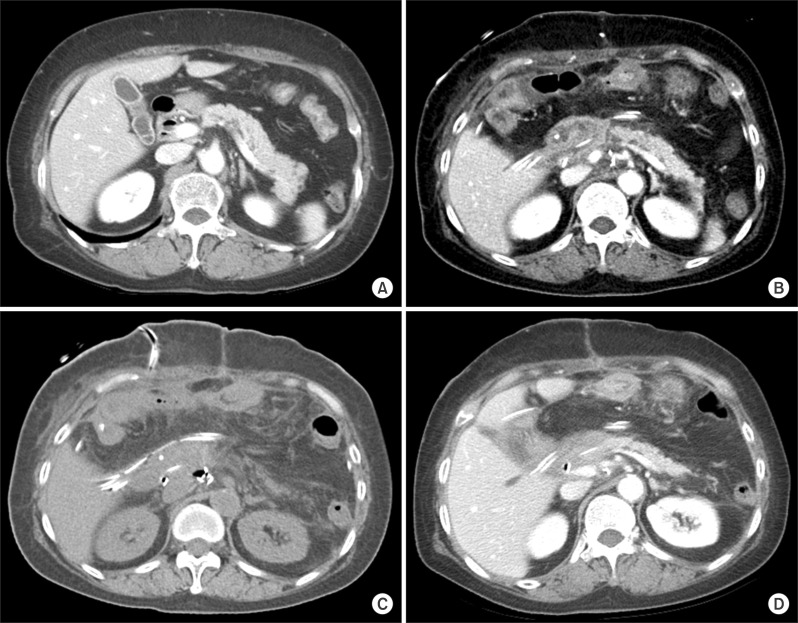 | Fig. 2Eventful sequences of trans-drain administration of excessively large amount of high-concentration antibiotics cocktail solution in a 72-year-female patient with ampulla of Vater cancer. High spiking fever occurred a few hours after trans-drain antibiotics administration. Computed tomography (CT) images are operative CT (A), 10-day CT image showing abnormal fluid collection around the pancreaticojejunostomy site (B), 11-day CT image showing mild diffuse local infiltration collection and scattered free air 1 day after trans-drain antibiotics administration (C), and 18-day CT image showing marked resolution of abnormal fluid collection 7 days after trans-drain antibiotics administration (D).
|
Go to :
DISCUSSION
PD has been regarded as the standard procedures for various malignant lesions in the periampullary region. Although the techniques of PD have improved considerably, some patients still experience surgical and medical complications. Postoperative diarrhea, steatorrhea, and poor nutritional status are frequent after PD. However, PJ leakage is the main cause of morbidity and mortality after PD. Pancreatic leakage can result in various kinds of surgical complications, including pseudoaneurysm and anastomotic disruption.1416 Pancreatic leakage is the most important cause of patient morbidity. It significantly contributes to prolonged hospitalization, increased health care costs, and mortality.19 Under normal conditions in adults, approximately 1,000 ml of pancreatic juice is excreted daily. We previously reported that the mean daily amount of excreted pancreatic juice after PPPD was 229±99 ml.1718 The amount of pancreatic juice is correlated with the volume of the remaining pancreas. It is reduced in patients with chronic pancreatitis. Other factors that can influence pancreatic leakage after PPPD include age, gender, preoperative jaundice, operative time, intraoperative blood loss, type of pancreatic reconstruction, anastomotic technique, consistency of the pancreatic stump, pancreatic duct diameter, use of somatostatin, and surgeon's experience.141920
Postoperative PF represents the failure of pancreatic-enteric anastomosis to heal or pancreatic parenchymal leak not directly related to pancreatic anastomosis.15 A diagnosis of postoperative PF is based on an amylase content >3 times of serum amylase activity on or after postoperative day 3. In addition, the finding of lipase activity ≥1,000 units/L in the abdominal drain showed high sensitivity and specificity for the diagnosis of PF.16 Therefore, we measured amylase and lipase concentrations in patient serum and abdominal drains on postoperative days 3 to 7 or longer. We also measured the volume of drainage fluid. To classify pancreatic leakage, fever, leukocytosis, prolonged drainage for 3 weeks, specific treatments including angiographic intervention, reoperation, death related to pancreatic leak, and readmission were investigated. Postoperative pancreatic leakage was graded according to the ISGPF. Compared to the invagination method, the duct-to-mucosa PJ method was found to be safer, with good duct patency and low pancreas atrophy.21 A meta-analysis showed that application of external pancreatic duct drainage after PD could decrease the incidence of pancreatic leakage when compared to the application without stent.22 A randomized controlled study also revealed that the external drainage of pancreatic juice was associated with lower overall postoperative morbidity rate and shorter hospital stay.23 In contrast, we previously reported that the incidences of PJ leak in our external group were similar to those in our internal drainage group.18
PJ leak lasting for 3 weeks can lead to the occurrence of other serious complications. If it is well controlled without evidence of infection, we can expect spontaneous cessation of pancreatic leak. In contrast, if it is infected and peripancreatic abscess is formed, it is difficult to treat effectively even if an abdominal drain is inserted in the right place. Medical treatment such as octreotide could not decrease the incidence of PF,4 although this remains controversial. It is also impossible or risky to insert a new percutaneous drainage tube at the operative site because of accidental bleeding and iatrogenic injury.
To cope with such infected pancreatic leak, we have searched for potential methods to control local infection. One of the major reasons to make the treatment of peripancreatic abscess difficult is that antibiotics cannot be effectively delivered into the inflammatory area because intravenous administration of antibiotics is only blood-borne. Thus, we thought of direct delivery of antibiotics into the peripancreatic abscess area. Since our antibiotics cocktail was highly concentrated, even one drop could make the local drug concentration easily reach their therapeutic level. Selection of antibiotics is one of the important points for this intraabdominal administration of antibiotics solution. Since we often encounter vancomycin-sensitive Staphylococcus aureus and imipenem-sensitive Escherichia coli in the drain discharge, we selected imipenem and vancomycin. If these antibiotics appear to be resistant in culture sensitivity test, other agents should be selected. The results of this study clearly demonstrated that direct delivery of antibiotics could be very effective to treat intractable peripancreatic abscess. Once local infection is treated, healing process is accelerated, leading to spontaneous closure of PF.
At first, we had worried out thpotential adverse side-effects of direct intraabdominal delivery of highly concentrated antibiotics. However, it appears to be acceptably safe based on the experience of this preliminary study. The only adverse effect observed was occurrence of febrile episode. This might be due to the wide spillage of infected fluid around the injection area. In one patient, after a relatively large amount of antibiotics cocktail solution was unintentionally injected, a definite febrile episode followed. Thus, we suggest that a small amount of antibiotics cocktail solution should be delivered to prevent unwanted wide spillage.
Our strategy in the management of PF after PD has evolved over time as in other surgical teams.4 Patients are given a liquid diet on postoperative day 7 under parenteral nutrition. It tolerated, they are advanced to a postgastrectomy diet on day 7 by tapering off parenteral nutrition. One day after the patient was placed on an oral diet, the amylase in the pancreatic drain was measured. We chose this time point because stimulation of the pancreas occurs after oral feeding. Such stimulation was significantly impaired in patients who underwent either PD or PPPD.17 If drain output was clear, we continued the oral feeding. CT scan showed that collections of fluid not drained, which might be infected and prevent the healing of PF. At this situation, we continued parenteral nutrition and light oral feeding. The patients in the control group were selected from an early study period. In contrast, the study group patients were gathered at the late phase of the study period because our strategy for the management of post-PD PF showed potential results.
The present study has several limitations. First, this is a retrospective preliminary single-center study. Therefore, our results may not be generalizable. Further validation of our result regarding the therapeutic efficacy and safety of high concentration of antibiotics is necessary using large patient populations from multiple centers.
In conclusion, the results of our study demonstrated that local trans-drain administration of antibiotics in patients showing intractable pus drainage after PD can be an effective therapeutic option for PJ leak-associated infection. Further validation of our result is necessary using large patient populations from multiple centers.
Go to :
 XML Download
XML Download