

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Liver transplantation (LT) has been accepted as an established treatment for end-stage liver diseases for the past three decades. Lifelong immunosuppression is essential for every LT recipient, but currently there are few institutional immunosuppression protocols that are applicable to recipients who survive for a long period of time.123 Thus, there is a real need to establish tailored, long-term, immunosuppressive regimens that are applicable to LT recipients and can be administered for life.
Posttransplant patient survival with good graft function for many years indicates the possibility of some immune tolerance.4 Withdrawing immunosuppression has been attempted by a small number of clinical trials, but most of these studies report similar conclusions, in that there is a low possibility of induced operational tolerance in current immunosuppressive clinical settings.5678 If there were some reliable methods for assessing immune function, they could be used for immune monitoring of operational tolerance and the tailored adjustment of immunosuppression protocols in LT recipients. Several specified bioassays, such as regulatory T-cell assays, helper T-cell assays, cytokine gene polymorphism assays, donor-specific antigen measurement, microarrays, and others are used for this purpose,4 but a reliable surrogate biomarker of immune tolerance has not been discovered.
Calcineurin inhibitors (CNIs), such as tacrolimus and cyclosporine, are the main immunosuppressive agents administered to LT recipients. CNIs upregulates calcineurin phosphatase (CNP) activity, by which the downregulation of calcineurin is induced and finally immunosuppressive effects develop.910 The CNI concentration is inversely correlated with calcineurin activity. The ImmuKnow assay uses the plant lectin phytohemagglutinin to stimulate lymphocyte activation. Most of the effector functions of immune cells depend on the cellular energy supply, and thus this assay is designed to measure the increase in intracellular adenosine triphosphate (ATP) following mitogen activation or recall antigenic or allogeneic stimulation. Because CNIs target T-cell function, CD4 cells are used for this assay.
In our present study, we assessed the clinical usability of the CNP activity assay and ImmuKnow assay as in vitro monitoring tools of immune cell function in adult LT recipients.
Go to : 
MATERIALS AND METHODS
Study design and patient selection
This prospective study was composed of 2 parts: independently applying the CNP activity assay or ImmuKnow assay to different study patients. All study patients were inpatients in the early posttransplant period, or readmission and outpatients undergoing routine follow-up after LT. The CNP activity assay was performed on 33 patients. These patients were selected according to their posttransplant period as follows: 15 recipients within 1 month after LT; 9 recipients after 1-12 months; 8 patients after 1-10 years; and 1 patient who had complete immunosuppression withdrawal for 10 years. All patients were administered tacrolimus at the time of blood sampling except one patient who had already completed immunosuppression withdrawal.
For the ImmuKnow assay, 118 young healthy individuals undergoing preoperative living-donor work-up were enrolled as a control group. The study group included 137 recipients who were selected according to the posttransplant period as follows: 77 recipients within 1 month after LT; 43 recipients within 1-12 months; and 17 patients within 1-10 years. All patients were administered tacrolimus at the time of blood sampling. Of these patients, 85 patients were also evaluated using the ImmuKnow assay a few days before LT.
For each assay, peripheral blood samples (5 ml) were collected in sodium heparin tubes on the day of blood collection. None of the results from these assays was used for clinical purposes, diagnosis, or treatment. The study protocol was approved by the institutional review board of Asan Medical Center (2014-0875).
Immunosuppression protocols
The peritransplant primary immunosuppression protocol that is administered to adult LT recipients at our institution consists of an interleukin-2 receptor inhibitor (basiliximab) on days 0 and 4; an intraoperative steroid bolus injection (5-10 mg/kg) and an intravenous or oral CNI and corticosteroid recycling starting on day 1; and adjunctive mycophenolate mofetil (MMF) for patients who develop CNI-associated adverse side effects or require additional immunosuppressive augmentation. Tacrolimus is usually preferred as the oral CNI, but patients with viral hepatitis C, hepatocellular carcinoma, or diabetes mellitus are often administered cyclosporine. Tacrolimus and cyclosporine are occasionally exchanged to control CNI associated adverse side effects. There are no differences in the immunosuppressive regimens administered to living-donor and deceased-donor LT recipients. Corticosteroids are rapidly tapered off within the first 3 months.
The target 12-hour trough concentrations for tacrolimus are around 12-15 ng/ml for the first 2 weeks; 12 ng/ml for 1-3 months; 8-10 ng/ml within 1 year; 7-8 ng/ml for 1-2 years; 5-6 ng/ml for 3-5 years; 4-5 ng/ml for 5-10 years; and 2-3 ng/ml after 10 years. Intentional withdrawal of all immunosuppressive agents was not considered in practice, except unusual situations such as serious infection. These tacrolimus target levels, especially for the first 3 months, are prudently adjusted according to the patient's condition, especially after living-donor LT with small-sized liver grafts because these recipients are often vulnerable to infection and acute rejection.
CNP activity assay
Blood samples were subsequently diluted with the same volume of phosphate-buffered saline solution in order to isolate the peripheral blood mononuclear cells using Ficoll-Paque Plus. The contaminating red blood cells were removed using a red blood cell lysis buffer. All isolation procedures are performed at room temperature within 12 hours after blood sampling. The collected mononuclear cells were lysed with ice-cold lysis buffer containing protease inhibitors. To objectively compare the CNP activity levels, we used 106 cells per assay. After centrifugation at 10,000 g for 10 minutes at 4℃, the resulting supernatants were used to measure CNP activity. The assay was performed using gamma-phosphorus 32 regulatory subunit type II phosphopeptide, which consists of 19 amino acids (Asp-Leu-Asp-Val-Pro-Ile-Pro-Gly-Arg-Phe-Asp-Arg-Arg-Val-Ser-Val-Ala-Ala-Glu), as the substrate. The total phosphatase activity was measured in a calcium (Ca) assay buffer that contained 2.5 mol/L calcium chloride and 500 mol/L okadaic acid in order to inhibit protein phosphatase types 1 and 2A. The radioactivity of 32-phosphorus released during 20 of minutes incubation is determined by liquid scintillation counting, and the phosphatase activity is expressed in terms of picomoles of phosphate released per minute per milligram protein. The background activity resulting from protein phosphatase type 2C - as measured in a Ca-free assay buffer containing 5.0-mmol/L EGTA (ethylene glycol-O,O-bis-[2-amino-ethyl]-N,N,N,N-tetra-acetic acid) instead of calcium chloride and 500 nmol/l okadaic acid under the same assay conditions used in the Ca assay buffer - is subtracted from the total phosphatase activity. The Ca-sensitive phosphatase activity is considered to be the CNP activity. We used a commercially available calorimetric CNP activity assay kit (Enzo, Farmingdale, NY). To compare the CNP activity levels objectively, 106 cells were used per assay in this study; thus, for convenience, we express CNP activity using a unit of 1 nmol/106 cells.
ImmuKnow assay
ImmuKnow is an immune cell function assay that detects cell-mediated immunity. The ImmuKnow assay detects cell-mediated immunity by measuring the concentration of ATP in CD4 cells following stimulation. ImmuKnow technology combines cell stimulation, cell selection, and the quantification of ATP as a metabolic marker in order to measure cell-mediated immunity. ImmuKnow measures early responses to stimulation by detecting intracellular ATP synthesis in CD4 cells that have been selected from the blood samples by monoclonal antibody-coated magnetic beads. The amount of ATP present in the stimulated blood specimens is a measure of lymphocyte activity. Since CD4 lymphocytes orchestrate cell-mediated immunity responses through immunoregulatory signaling, the measurement of CD4 activation reflects the degree of immune function. Its limit of ATP detection is 1 ng/ml. The ATP level ranges determined by the ImmuKnow assay were established by testing 155 apparently healthy adults and 127 transplant recipients. The cumulative frequency of the differences was used to select the ATP levels that give the best balance of the results between immunosuppressed and non-immunosuppressed individuals. The cutoff levels used for the ATP level ranges were 225 and 525 ng/ml. Thus, the results were interpreted as follows: low immune response (ATP level ≤225 ng/ml); moderate immune response (ATP level 226-524 ng/ml); and strong immune response (ATP level ≥525 ng/ml). We used the ImmuKnow kit (Cylex Inc., Columbia, MD; currently, Viracor-IBT laboratories, Lee's Summit, MO).
Statistical analysis
The continuous variables are presented as the mean±SD or median. The student t-test was used for comparisons. In this study, p<0.05 was considered statistically significant. Simple linear regression analysis is presented with a regression equation, correlation coefficient (r), and coefficient of determination (r2). Statistical analyses were performed using GraphPad Prism (version 5.0; GraphPad, La Jolla, CA), SPSS (version 20; IBM, New York, NY), and Statistica software (version 6.0; StatSoft, Tulsa, OK).
Go to :
RESULTS
CNP activity in LT recipients
The demographic profiles of the 33 patients who were evaluated using the CNP activity assay are summarized in Table 1. The types of LT included living-donor LT in 27 patients and deceased-donor LT in 6 patients. Six patients received ABO blood group-incompatible living-donor LT. The primary administered immunosuppressant included tacrolimus in all recipients, except 1 case of immunosuppression withdrawal, and 17 recipients (51.5%) also received adjunctive MMF. All of these patients demonstrated stable liver function at the time of blood sampling.
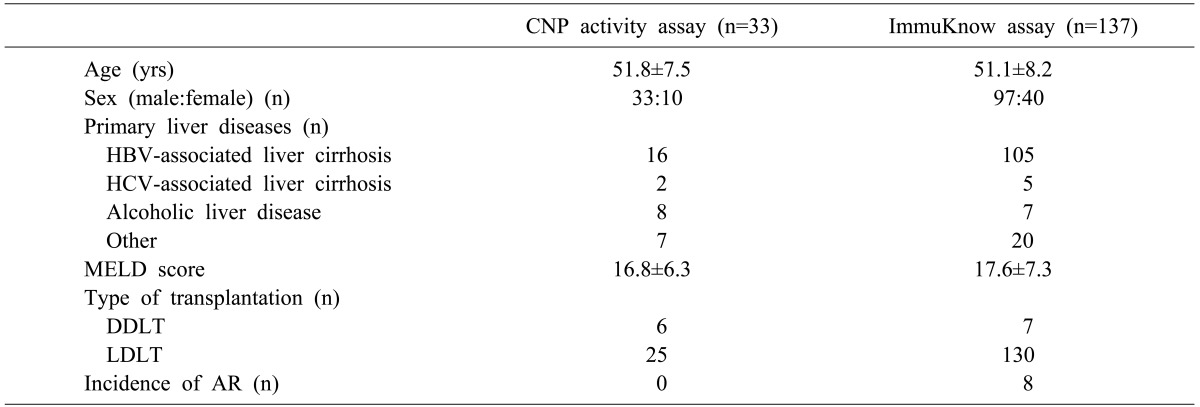
The correlation between the 12-hour trough concentration of tacrolimus and CNP activity in all 33 patients is depicted in Fig. 1, which demonstrated a rough linear correlation (r=0.436; r20.191; p=0.011; y=1.22+0.21*x). The patients were divided into 2 groups according to use of adjunctive MMF. Among the 17 patients who were administered tacrolimus and MMF, there was no correlation between tacrolimus concentration and CNP activity (r=0.087; r20.008; p=0.739; y=2.78+0.06*x) (Fig. 2A). The mean 12-hour trough concentration of mycophenolic acid was 1.8±0.9 µg/ml (range=0.3-3.7). In contrast, among the 15 patients who were only administered tacrolimus, there was a significant linear correlation between tacrolimus concentration and CNP activity (r=0.803; r20.644; p=0.0003; y=0.23+0.27*x) (Fig. 2B).
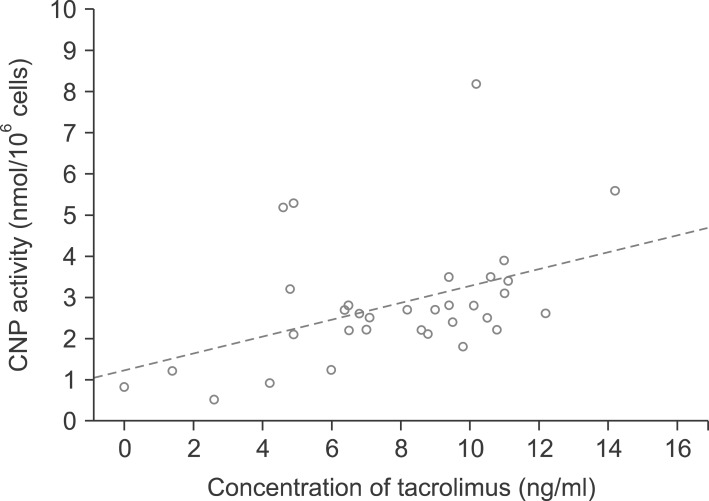 | Fig. 1Scatterplot graph showing the correlation between the 12-hour trough tacrolimus concentration and calcineurin phosphatase (CNP) activity in 33 patients. The dotted line indicates the regression equation.
|
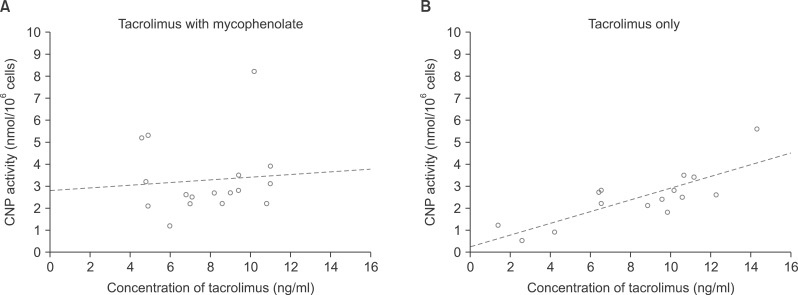 | Fig. 2Scatterplot graphs showing the correlation between the 12-hour trough tacrolimus concentration and calcineurin phosphatase (CNP) activity in (A) 17 patients who were administered tacrolimus and mycophenolate mofetil and (B) 15 patients who were administered only tacrolimus. The dotted lines indicate the regression equations.
|
The patient who withdrew from receiving immunosuppression was a 60-year-old male patient who underwent deceased-donor LT outside of Korea 23 years prior. He had arbitrarily ceased receiving immunosuppression (tacrolimus) 10 years prior and was relatively healthy until 3 months before enrollment. This sequence indicates the development of spontaneous operational tolerance. However, he was admitted due to the sudden development of multiple liver abscesses and diffuse ischemic damage in the intrahepatic bile ducts due to the complete occlusion of the hepatic artery. One month later, compensatory arterial collaterals formed very slowly. At first, we thought that such unusual arterial occlusion was associated with some adverse immunological reaction, but the spontaneous development of arterial collaterals indicates the presence of operational tolerance. We did not administer CNI due to the high risk of ongoing infection, and thus his CNP activity was measured as low as 0.8 nmol/106 cells.
ImmuKnow results in healthy individuals
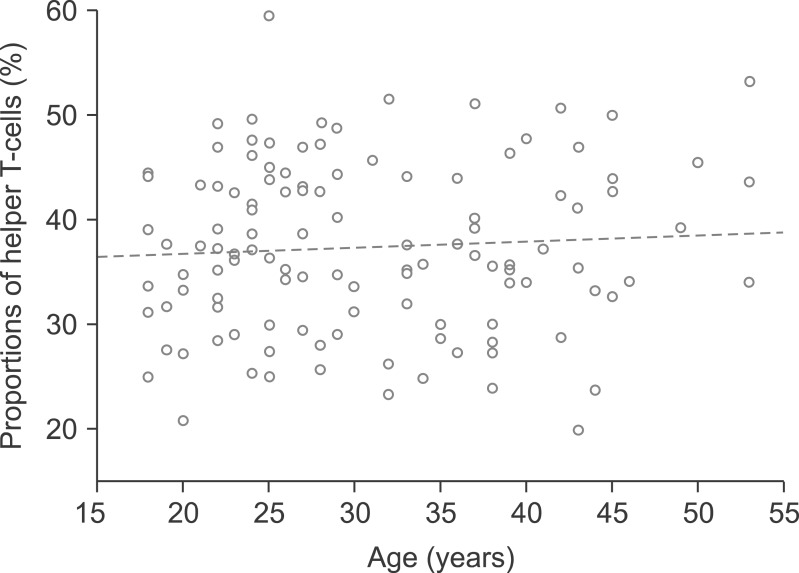
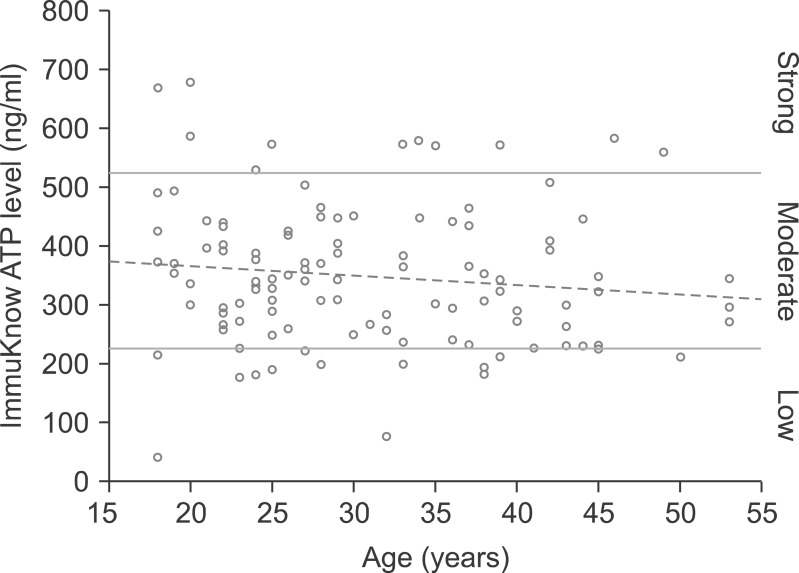
Immune cell function was evaluated in healthy individuals who comprised the control group. The 118 living-donor candidates consisted of 76 males (64.4%) and 42 females (35.6%), who demonstrated a mean age 30.7±9.2 years (range: 18-53 years). The distributions of the proportions of helper T-cells according to age are depicted in Fig. 3, and there were no significant changes associated with increasing age (r=0.064; r20.004; p=0.491; y=35.65+0.06*x). The mean proportion of helper T-cells was 37.4±8.1%. The distribution of ImmuKnow ATP levels according to age is also shown in Fig. 4, and there was no significant change associated with age (r=-0.123; r20.015; p=0.183; y=397.68-1.61*x). According to the predefined ImmuKnow criteria, 12 patients (10.2%) demonstrated a strong immune response, 92 patients (78.0%) demonstrated a moderate response, and 14 patients (11.9%) demonstrated a low response.
The healthy individuals were divided into 2 groups according to sex. Among the 76 male patients, the distribution of ImmuKnow ATP levels according to age is shown in Fig. 5A, but there was no significant change associated with age (r=-0.059; r20.004; p=0.611; y=383.15 -0.76*x). The immune responses in these male patients were classified as strong in 10 patients (13.2%), moderate in 61 patients (80.3%), and low in 5 patients (6.6%). Among 42 female patients, the distribution of ImmuKnow ATP levels according to age is also depicted in Fig. 5B, but there was also no significant change associated with age (r=-0.198; r20.039; p=0.183; y=414.16-2.72*x). The immune responses in female patients were classified as strong in 2 patients (4.8%), moderate in 31 patients (73.8%), and low in 9 patients (21.4%). There were no differences in ImmuKnow ATP levels between healthy male and female patients (360.6±119.4 ng/ml in male patients vs 325.5±114.1 ng/ml in female patients; p=0.122).

ImmuKnow assay results in patients with end-stage liver disease waiting for LT
The ImmuKnow assay was performed on 85 adult patients with end-stage liver disease waiting for LT. All of these patients underwent LT within 2 weeks. The distribution of ImmuKnow ATP levels according to age is depicted in Fig. 6, and there was a significant change with age (r=-0.342; r20.117; p=0.001; y=244.29-2.92*x). The immune responses were classified as strong in none of the patients (0%), moderate in 8 patients (9.4%), and low in 77 patients (90.6%). There was a definite difference in ImmuKnow ATP levels between the healthy individuals and patients with end-stage liver diseases (347.4±116.1 ng/ml in healthy individuals vs 96.0±82.7 ng/ml in liver disease patients; p=0.000).

ImmuKnow assay results in LT recipients
The ImmuKnow assay was performed on 137 adult LT recipients, and their profiles are summarized at Table 1. The primary immunosuppressant administered to all recipients was tacrolimus, and 73 patients (53.3%) received adjunctive MMF. The ImmuKnow assay was performed 543 times on these 137 recipients (mean 4.0 times). In total, the ImmuKnow assay was performed 212 times on 73 patients who were receiving both tacrolimus and MMF (mean 2.9 times) and 331 times on 64 recipients who were administered only tacrolimus (mean 5.2 times).
The distribution of ImmuKnow ATP levels according to the 12-hour trough concentrations of tacrolimus is also shown in Fig. 7, but there was no correlation between the ImmuKnow ATP level and tacrolimus concentration (r=-0.023; r20.001; p=0.601; y=210.48+0.72*x).
 | Fig. 7Scatterplot graph showing the distribution of ImmuKnow ATP levels according to the 12-hour trough tacrolimus concentration in 137 liver transplant recipients. The ImmuKnow assay was performed 543 times on these 137 patients (mean 4 times). In the right column, the ranges of immune responses are depicted. The dotted line indicates the regression equation.
|
The recipients were divided into 2 groups according to use of adjunctive MMF. Among 73 patients who were administered tacrolimus and MMF, the distribution of ImmuKnow ATP levels did not show a correlation with tacrolimus concentration (r=-0.017; r20.0003; p=0.809; y=247.07+0.71*x) (Fig. 8A). The mean 12-hour trough concentration of mycophenolic acid was 0.9±0.6 "g/ml (range =0.3-4.4). Among 64 patients who were only administered tacrolimus, the distribution of ImmuKnow ATP levels also did not show a correlation with the tacrolimus concentration (r=-0.030; r20.0009; p=0.583; y=186.3+0.79*x) (Fig. 8B).
 | Fig. 8Scatterplot graphs showing the distributions of ImmuKnow ATP levels according to the 12-hour trough tacrolimus concentrations in (A) 73 patients who were administered tacrolimus and mycophenolate mofetil and (B) 64 patients who were only administered tacrolimus. The dotted lines indicate the regression equations.
|
Eight recipients experienced clinically suspected or biopsy-proven acute rejections at the time of blood sampling. Their median ATP concentration according to the ImmuKnow assay was 298.3 ng/ml, and none demonstrated a strong immune response.
Go to :
DISCUSSION
Immune tolerance has long been regarded as the "holy grail" of organ transplantation, and many clinicians and immunologists have made enthusiastic efforts to achieve this goal. Over the past two decades, the accumulating evidence suggests that clinical operational tolerance is rare but achievable following LT. The long-term success of clinical operational tolerance has only been realized in a few LT recipients via developing mixed chimera or antibody induction therapies followed by stepwise weaning of immunosuppression under strict monitoring.45678 Some patients have also developed spontaneous operational tolerance due to non-compliance with immunosuppressant medication. One patient in this present study with total hepatic artery occlusion demonstrated such spontaneous operational tolerance, although we do not know if it will be uneventfully maintained for the remainder of the patient's life. A noticeably low level of CNP activity without CNI immunosuppression indicates that CNP activity may not be associated with the induction of spontaneous operational tolerance in this recipient.
In order to understand the mechanisms of immune tolerance and optimize immunosuppression, monitoring of functional immunity is essential in LT recipients. Monitoring of functional immunity may help appropriately manage such patients and avoid acute rejection, the side effects of drugs, and infections. Effective biomarkers of operational tolerance would make the minimization of immunosuppression more successful. Implementing drug minimization can only be safely and reliably achieved when guided by means that reflect the individual's immune condition. It is now well accepted that the laboratory tests that are routinely performed to assess graft function are not highly sensitive to graft injury. With better understanding of the cellular and molecular mechanisms of transplantation tolerance, novel immunological markers and assays are starting to emerge as invaluable assets for tolerance monitoring.4
Fukudo et al.9 compared the pharmacodynamic properties of CNIs in rats in order to clarify different therapeutic drug monitoring strategies in clinical situations. The time profiles of blood concentrations and calcineurin activities in whole blood samples obtained from rats were examined after the single or repeated administrations of each drug. A substantial time delay in inhibition was observed following the single administration of CNI, thereby resulting in anticlockwise hysteresis in the relationship between blood concentrations and calcineurin inhibition in whole blood. In contrast, such a hysteresis loop diminished after the repeated administration of CNI. Distinct pharmacodynamics may partly contribute to the therapeutic drug monitoring strategy in transplant patients receiving CNI.
CNIs have been widely administered after LT for a long time. Since these drugs have a narrow therapeutic range and show large inter- and intraindividual pharmacokinetic variabilities, frequent therapeutic drug monitoring is required to control their blood concentrations. Even when the blood concentrations are within the therapeutic range, some patients still experience acute rejection or infections. CNIs form a complex with their respective binding proteins, immunophilins, which in turn inhibit the phosphatase activity of calcineurin, which is a key enzyme involved in the activation of T-cells.11 Pharmacodynamic assessment of CNP activity in combination with monitoring blood concentrations has also been studied. The inhibitory effects on calcineurin activity in peripheral blood mononuclear cells differs between tacrolimus and cyclosporine in LT recipients. The pharmacodynamics of CNIs demonstrate great inter- and intraindividual variations, and acute rejection is associated with calcineurin activity. Calcineurin activity at the trough time points has been suggested as a single surrogate predictor of overall calcineurin activity throughout the dosing periods. Monitoring CNP activity might be useful for determining the therapeutic ranges of the tacrolimus and cyclosporine concentrations in individual patients who have been treated with CNI.12131415 Measuring CNP activity appears to be beneficial for determining the level of immunosuppression, but it takes a relatively long time and requires complex laboratory procedures. Thus, the CNP activity assay is only readily performed in laboratory settings, not in the routine clinical setting.
Interestingly, the results of our present study show that CNP activity is closely correlated with tacrolimus concentration, but this correlation became disrupted when MMF was concurrently administered. We speculate from this that MMF is involved in unknown mechanisms that affect calcineurin metabolism. In our present analysis, the inhibition of the enterohepatic cycle during cyclosporine co-administration explains some of the differences observed in the pharmacokinetics of MMF when co-administered with either tacrolimus or cyclosporine.16 The co-administration of cyclosporine or tacrolimus differently affects the therapeutic drug monitoring of mycophenolic acid. The concurrent use of tacrolimus may decrease the mycophenolic acid concentration, thereby leading to an increased dose of MMF.1718 Contradictory results have also been reported, in that co-administration with cyclosporine required significantly higher doses of MMF to achieve similar mycophenolic acid levels as tacrolimus-treated patients.19 It has also been suggested that the cyclosporine-mediated inhibition of the biliary excretion of mycophenolic acid glucuronide by the multidrug resistance-associated protein-2 transporter is the mechanism responsible for the interactions between cyclosporine and MMF.20
The ImmuKnow assay is specifically designed to assess the overall immune response in patients receiving immunosuppressive agents, and thus quantitatively estimate the risks of acute rejection and infection. As expected, we found very wide ranges of inter- and intraindividual variations in ImmuKnow ATP levels, even in healthy individuals.12212223 It may be natural for seriously ill patients with end-stage liver disease who are awaiting LT to demonstrate unusually low immune responses, especially after considering their very poor general conditions and associated systemic derangement. It is a unique finding that the ImmuKnow ATP levels were elevated soon after LT, despite vigorous immunosuppression. We could not find a significant correlation between the ImmuKnow ATP level and tacrolimus concentration. The incidence of clinically suspected or biopsy-proven acute rejection was relatively low in our study patients, and thus it was not possible to determine if a strong immune response was closely associated with the development of acute rejection, or if a low immune response is related to the decreased occurrence of acute rejection.12 Our current results indicate that the posttransplant assessment of immune responses using the ImmuKnow assay is not sufficiently reliable for predicting the occurrence of acute rejection or other adverse events.
LT is frequently performed on patients with hepatocellular carcinoma, and customized long-term immunosuppressive regimens need to be developed to help prevent hepatocellular carcinoma recurrence and post-recurrence treatment.24 Tailored immunosuppressive regimens that cover the long-term posttransplant period should be established after considering individual patient profiles, including the diagnosis of hepatocellular carcinoma.
Based on the results of our present study, we conclude that the roles of the CNP activity assay and ImmuKnow assay are too limited to objectively determine the level of immune cell function. Thus, we think that there is no practical need to perform these bioassays on LT recipients as methods for determining the level of immunosuppression. Further studies should be performed to identify other diagnostic methods that would enable predictive immune function monitoring.
Go to :
 XML Download
XML Download