

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Distal pancreatectomy is performed for various benign and malignant pancreatic disease.1 Whether in pancreaticoduodenectomy or distal pancreatectomy, postoperative pancreatic fistula is still regarded as a major complication.2 Pancreatic fistula (PF) is asymptomatic in many patients, but it may precipitate clinically relevant complications including intra-abdominal abscess, hemorrhage and sepsis.3
According to the International Study Group of Pancreatic Fistula (ISGPF),4 PF is diagnosed when there is measurable drain output on or after postoperative (POD) 3 days, with an amylase content 3 times the upper limit of normal serum value. The ISGPF has proposed a classification scheme for PF based on clinical and laboratory parameters, but it has not been correlated with laboratory results and clinical course.5
Although clinical studies regarding PF after pancreaticoduodenectomy have been reported, the incidence and clinical course of PF after distal pancreatectomy have not been well investigated.5,6,7,8,9 Pancreatic lipase is also representative pancreas enzymes, but the ISGPF used only amylase concentration in the drain by expert opinions without explanation.
Therefore, the first aim of this study was to compare the predictability for clinical PF between drain amylase and lipase. The second aim was to evaluate the appropriate postoperative day (POD) for use as the diagnostic criterion of PF with clinical relevance.
Go to : 
MATERIALS AND METHODS
Patients
Between March 2010 and March 2014, a total of 154 patients underwent distal pancreatectomy at Yonsei Universty Health System, Gangnam Severance Hospital and Severance Hospital. All cancer patients were staged according to the 7th edition of American Joint Committee on Cancer staging system (AJCC).
The surgical procedures and perioperative management were performed as previously reported.10 Drains were used routinely in all patients and were placed in the resected stump of the pancreas. The drain fluid was daily collected and quantitatively analyzed for amylase and lipase content. The criteria for drain removal was the output was <100 ml/day for consecutive days or lack of PF, as well as absence of abnormal fluid collection, abscess or infection.
Diagnostic criterion PF
The receiver operating characteristics (ROC) curve of drain amylase or lipase concentration on each day was used to predict clinical PF (ISGPF grade B or C). To evaluate the appropriate POD to use as the diagnostic criterion of PF with clinical relevance, the AUC of ROC curve of drain amylase concentration on each day were compared. We considered the day for diagnostic criterion for PF POD with the most precise prediction of clinical PF (AUC closest to 1), and then modified the definition of ISGPF to reduce the clinically irrelevant PF (ISGPF grade A).
Statistical analysis
The ROC curve analysis of the drainage amylase concentration on each day and AUC value was used to predict the clinical PF (ISGPF grade B or C). R package, version 3.0.2 (http://www.R-project.org) was used to perform these analyses.
Go to :
RESULTS
Patients Characteristics
A total of 154 patients who underwent distal pancreatectomy were included in this study. The study group consisted of 67 men and 87 women whose mean age was 61.5±10.5 years. Of the 154 patients, 110 underwent open distal pancreatectomy, 38 underwent laparoscopic distal pancreatectomy, and 6 underwent robotic distal pancreatectomy. Their pathologic diagnoses were pancreatic carcinoma in 44, solid pseudopapillary tumor of pancreas in 26, neuroendocrine tumors in 23, mucinous cystic neoplasm in 17, pseudocyst in 16, intraductal papillary mucinous neoplasm in 12, metastatic cancer in 10, and pancreatic injury in 6 patients.
Of these 154 patients, PF developed in 76 (49.3%) patients. Grade A pancreatic fistula occurred in 49 (31.8%) patients, grade B in 24 (15.6%) patients, and grade C in 3 (1.9%) patients.
Predictability for clinical PF between drain amylase and lipase
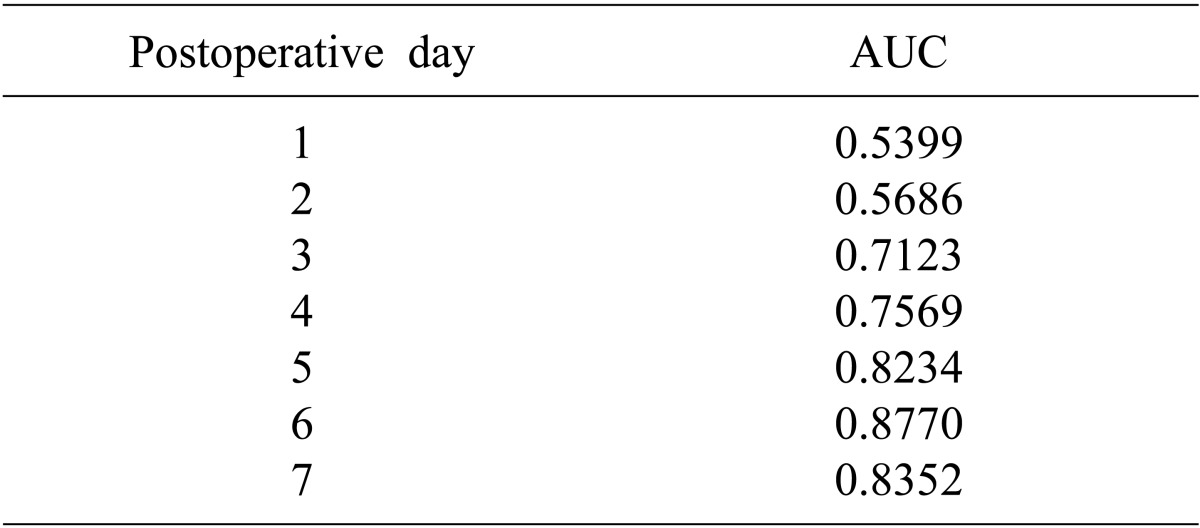
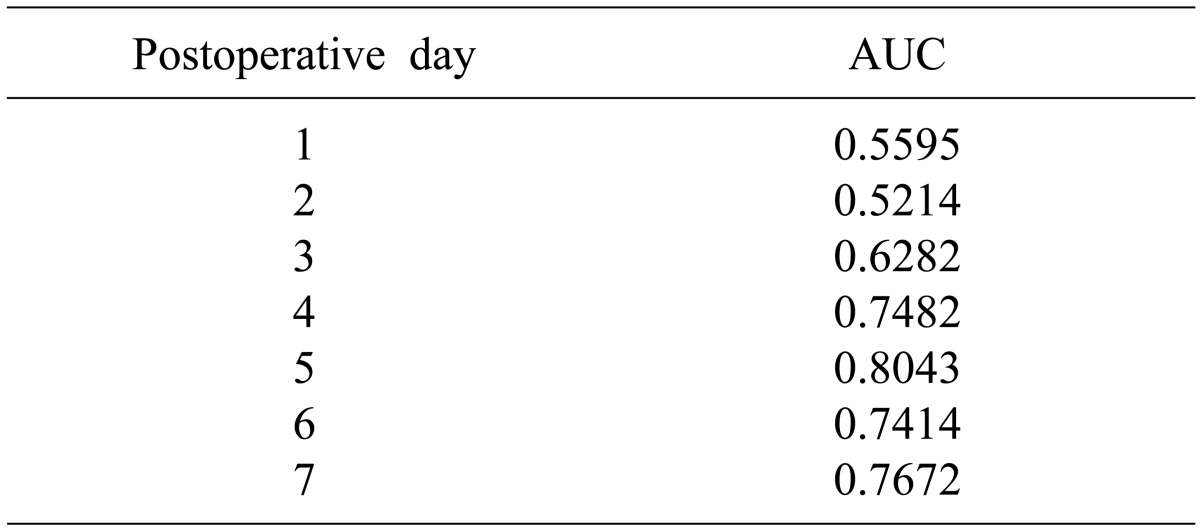
The AUC values of drain concentration for amylase poorly predicted clinical PF before POD 3, but became well correlated with clinical PF (ISGPF grade B or C) after POD 5 (Table 1). The AUC values of lipase poorly predicted clinical PF before POD 3, but was also well correlated with clinical PF after POD 5 (Table 2). In contrast, the prediction of clinical PF using drain lipase did not different from that using drain amylase.
The day for diagnostic criterion for PF
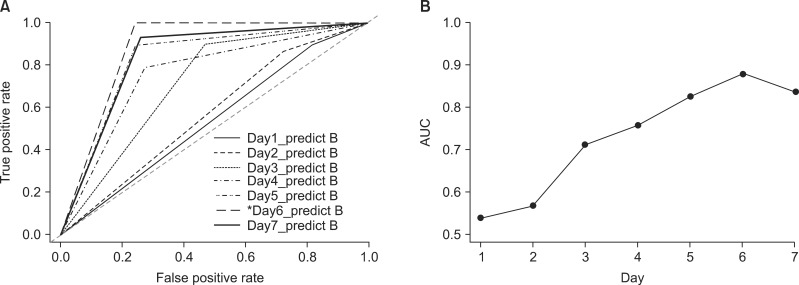
AUC of ROC analysis showed that drain pancreatic enzyme measurement POD 6 was the most appropriate diagnostic criterion for postoperative PF (Fig 1).
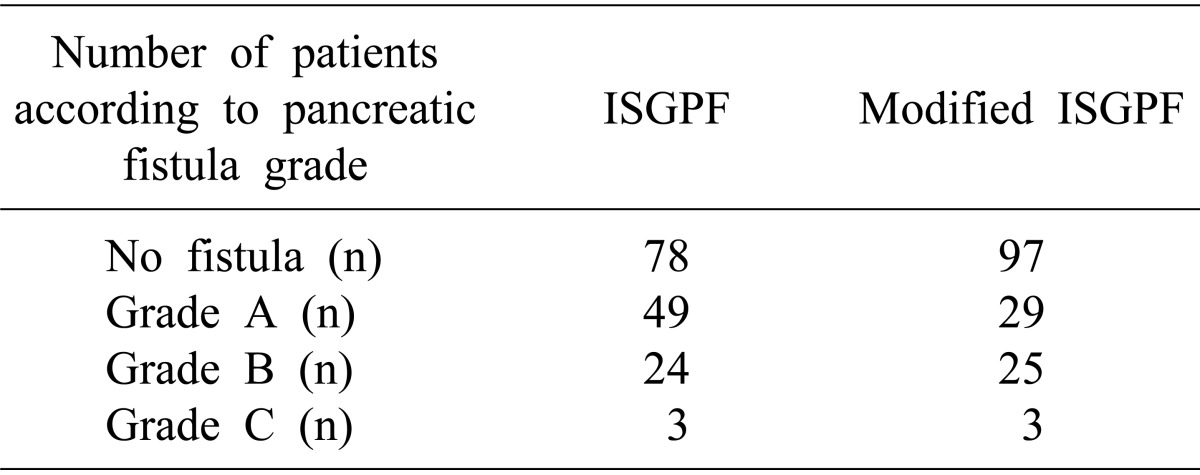
We used the value on POD 6 to predict clinical PF and then modified the definition of ISGPF, and then defined the criterion as an amylase concentration greater than three times that of normal upper limit. After this modification of ISGPF, the number of patients with the clinically irrelevant PF (grade A) were reduced from 49 to 29, but the incidence of clinical PF was not changed (Table 3).
Go to :
DISCUSSION
The ISGPF defines PF by amylase concentration but does not explain why it alone was chosen. Lipase is more accurate parameter than amylase for the diagnosis of acute pancreatitis.11,12 Due to this point, the use of lipase for the diagnosis of postoperative PF was investigated in this study. There was one study reporting that the lipase level in the drainage fluid is more sensitive parameter for prediction of clinical complications with pancreatic leakage than amylase concentration in gastrectomy.13 In this study, clinical PF was strongly correlated lipase concentrations in the drains. Therefore, measurement of lipase concentration would have some diagnostic significance for clinical PF.
The purpose of the present study was to determine if modified definition for PF can be used to predict which patients will develop a clinically significant PF. This question is important because current ISGPF may increase the rate of clinical irrelevance PF (grade A). In this study, the number of patients with clinically irrelevant or laboratory PF (grade A) according to modified ISGPF definition was reduced from 49 to 29 after modification of PF definition. In previous studies, amylase concentration was elevated during the early postoperative period and then gradually decreased to nearly normal levels by POD 4 in most patients.10 However, in the clinical postoperative PF group, the drain amylase concentration was continuously high or re-elevated due to failure of healing process and followed a bimodal distribution during the postoperative period. This may explain why the values on POD 6 were more closely correlated with PF than those on POD 3.
This study has limitations that performed retrospectively and was not verified to other clinical settings. Nonetheless, it showed that the predictability for clinical PF was assessed between drain amylase and lipase, and that POD 6 value was appropriate as a diagnostic criterion of PF with clinical relevance after distal pancreatectomy. Modification of the current ISGPF classification may be needed to improve the clinical correlation with the pancreatic enzyme drain concentrations during the postoperative period, especially in patients undergoing distal pancreatectomy.
Go to :
 XML Download
XML Download