

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Since its introduction, laparoscopic cholecystectomy has become the gold standard treatment for gallstone disease.1 However, the incidence rate of bile duct injury (BDI) has risen from 0.06% to 0.3%. Open cholecystectomy has risen from 0.5% to 1.4% when gallbladder removal is performed laparoscopically.2,3,4,5,6,7,8,9,10,11,12 In initial studies on the removal of laparoscopic gallbladder, complications such as bleeding, wound infection, respiratory insufficiency, trocar injury to the intra-abdominal viscera, major vascular injury, and bile leaking accounted for reported morbidity rate ranging from 1.0% to 8.0%.2,3,4,5,6,7,8 Despite the completion of the learning curve and the recognition of preventive maneuvers to avoid ductal injury during laparoscopic cholecystectomy, the incidence rate of BDI remains unchanged.13 In addition, injuries of the bile duct system after laparoscopic cholecystectomy are more complex than that after an open approach, causing significant morbidity and even death. Associated vascular lesions, particularly injuries to the right hepatic artery or longitudinal strictures of the common bile duct due to failed repair attempts, are not uncommon. Various classifications of bile duct injuries after laparoscopic cholecystectomy were reviewed in this article.
Go to : 
CLASSIFICATION OF BILE DUCT INJURY
Bismuth classification
The first classification of bile duct injury is authored by H. Bismuth in 1982. Up to now, a number of classifications have been proposed by different authors. The Bismuth classification is a simple classification based on the location of the injury in the biliary tract. This classification is very helpful in prognosis after repair. This classification included five types of bile duct injuries according to the distance from the hilar structure especially bile duct bifurcation, the level of injury, the involvement of bile duct bifurcation, and individual right sectoral duct.14 Type I involves the common bile duct and low common hepatic duct (CHD) >2 cm from the hepatic duct confluence. Type II involves the proximal CHD <2 cm from the confluence. Type IIIis hilar injury with no residual CHD confluence intact. Type IV is destruction of the confluence when the right and left hepatic ducts become separate. Type Vinvolves the aberrant right sectoral hepatic duct alone or with concomitant injury of CHD. However, the Bismuth classification does not include the wide spectrum of possible biliary injuries.
Strasberg classification
The Strasberg classification is a modification of the Bismuth classification, but allows differentiation between small (bile leakage from the cystic duct or aberrant right sectoral branch) and serious injuries performed during laparoscopic cholecystectomy as type A to D. Type E of the Strasberg classification is an analogue of the Bismuth classification.3 The Strasberg classification, summarized in Fig. 1, is very simple which can be easily applied to bile duct injuries. The major disadvantage of the Strasberg classification is that it does not describe additional vascular involvement at all. For this reason, the Strasberg classification could not demonstrate a significant association between the discrimination of specific injury patterns and the resection of liver tissues.
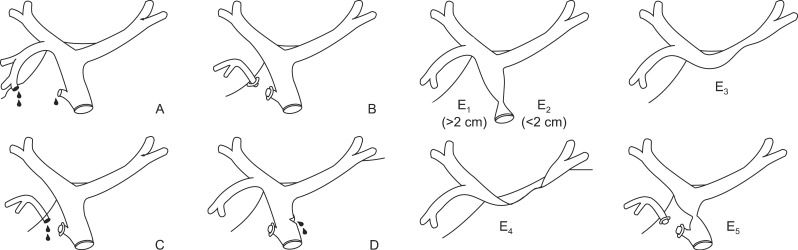 | Fig. 1Strasberg classification.3,22 (A) Bile leak from cystic duct stump or minor biliary radical in gallbladder fossa. (B) Occluded right posterior sectoral duct. (C) Bile leak from divided right posterior sectoral duct. (D) Bile leak from main bile duct without major tissue loss. (E1) Transected main bile duct with a stricture more than 2 cm from the hilus. (E2) Transected main bile duct with a stricture less than 2 cm from the hilus. (E3) Stricture of the hilus with right and left ducts in communication. (E4) Stricture of the hilus with separation of right and left ducts. (E5) Stricture of the main bile duct and the right posterior sectoral duct.
|
McMahon classification
McMahon et al. proposed another classification of bile duct injuries after laparoscopic cholecystectomy. They classified the injury by the width of bile duct injury. Based on the McMahon classification, lacerations under 25% of the common bile duct (CBD) diameter or cystic-CBD junction was classified as minor injury, whereas transection or laceration over 25% of CBD diameter and postoperative bile duct stricture were classified as major injury.2
Stewart-Way classification
Bile duct injuries fall into four classes based on the Stewart-Way classification.15 Class I injury occurs when CBD is mistaken for the cystic duct, but the error is recognized before CBD is divided. Class II injuries involve damage to CHD from clips or cautery used too close to the duct. This often occurs in cases where visibility is limited due to inflammation or bleeding. Class III injury, the most common type, occurs when CBD is mistaken for the cystic duct. The common duct is transected and a variable portion including the junction of the cystic and common duct is excised or removed. Class IV injuries involve damage to the right hepatic duct (RHD), either because this structure is mistaken for the cystic duct, or because it is injured during dissection (Fig. 2). Both complex bileduct and vascular injuries were included in the Stewart-Way classification.
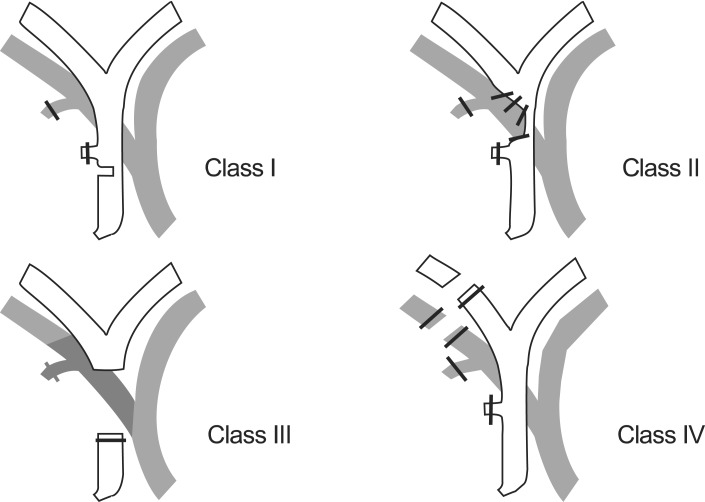 | Fig. 2Stewart-Way classification.15
|
Hannover classification
Bektas et al. proposed a new classification system named Hannover classification after comparing the classification of bile duct injury for consecutive 72 iatrogenic bile injuries after laparoscopic cholecystectomy. In the Hannover, bile duct injuries were divided into five types from A to E.16 Type A is peripheral bile leakage. Type B is stricture of CHD or CBD without injury. Type C is lateral CHD or CBD injury. Type D is total transection of CHD. Type E is bile duct stricture of the main bile duct without bile leakage at postoperative state. Vascular injuries are included in Type C and Type D (Fig. 3). The Hannover classification distinguished a total of 21 injury patterns in a small group of patients. The advantage of the Hannover classification is that it has a high level of statistical significance to demonstrate the association between the discrimination of classifiable injury patterns and the surgical treatments chosen. Other classification systems could only distinguish fewer injury patterns. Furthermore, with the Hannover classification, there were significant associations between the discrimination of specific injury patterns and the resection of liver tissue as well as resection of the bifurcation of the hepatic duct. The advantage of the Neuhaus' classification may be the ability to discriminate different injury patterns and recurrent cholangitis in the long-term. This Hannover classification provides discriminators for the localization of tangentially or completely transected bile ducts above or below the bifurcation of the hepatic duct, which is a major drawback of other classification systems.
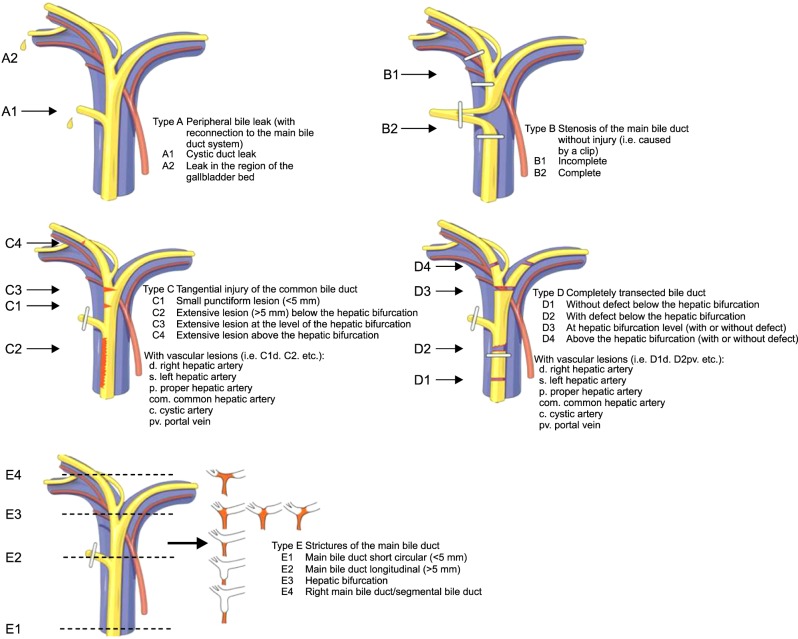 | Fig. 3Hannover classification.16
|
Mattox classification
The Mattox classification of BDI takes into consideration the types of injuring factors (contusion, laceration, perforation, transection, diversion or interruption of the bile duct or the gallbladder).17 There are several classifications in the literature for induced BDI during laparoscopic cholecystectomy (Schmidt et al.,18 Bergman et al.,19 Csencdes et al.,20 and Lau et al.21).
Go to :
 XML Download
XML Download