

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Intraductal papillary mucinous neoplasms (IPMNs) of the pancreas have been increasingly diagnosed due to the widespread use of advanced imaging modalities such as computed tomography (CT) and magnetic resonance imaging (MRI). IPMNs are typically classified into three groups: main duct type IPMN (MD-IPMN), branch duct type IPMN (BD-IPMN), and mixed type IPMN. In 2012, the international consensus guidelines for the management of IPMNs have been revised by the working group of the International Association of Pancreatology (IAP) following the 14th meeting of the IAP (Fukuoka, Japan in 20101). Despite some limitations in predicting malignant BD-IPMN,2 the utility of these guidelines for management of BD-IPMN has been validated by some studies.3,4
For MD-IPMNs, surgical resection is strongly recommended for all patients. However, management of BD-IPMNs is still controversial. Due to lower possibility of malignancy in BD-IPMNs (reported as about 25%1), surgical resection of BD-IPMNs is only considered for selected patients. In patients with multifocal BD-IPMNs (14.5-41%5,6 of BD-IPMNs are known to be multifocal), the extent of pancreatic resection needs to be determined carefully considering both the risk of tumor progression from BD-IPMNs in the remnant pancreas and the reduction of quality of life from aggressive resection with curative intent.
In this study, we evaluated the surgical outcomes of multifocal BD-IPMNs after resection. The long-term result of the remnant pancreas in these patients were followed-up. We especially investigated whether we could safely preserve parenchyma of the pancreas that had multifocal BD-IPMNs.
Go to : 
MATERIALS AND METHODS
Between January 1995 and December 2013, 699 patients underwent pancreatic resection for IPMN of the pancreas at the Department of Surgery in Asan Medical Center. The diagnosis of IPMN was confirmed by pathologic result for all cases. Among them, 337 patients had BD-IPMN. Of the 337 patients, 37 showed multifocality. Because the purpose of this study was to review the prognosis and fate of remaining pancreas with BD-IPMNs, we excluded 15 patients whose multifocal BD-IPMNs were completely removed through pancreatic resection (which means no residual BD-IPMNs in the remnant pancreas). Patient selection flow is illustrated at Fig. 1. Medical records of 22 patients who still had BD-IPMNs (with or without mixed type IPMNs) were retrospectively reviewed, including past medical histories, radiologic findings, laboratory data, and pathologic results.
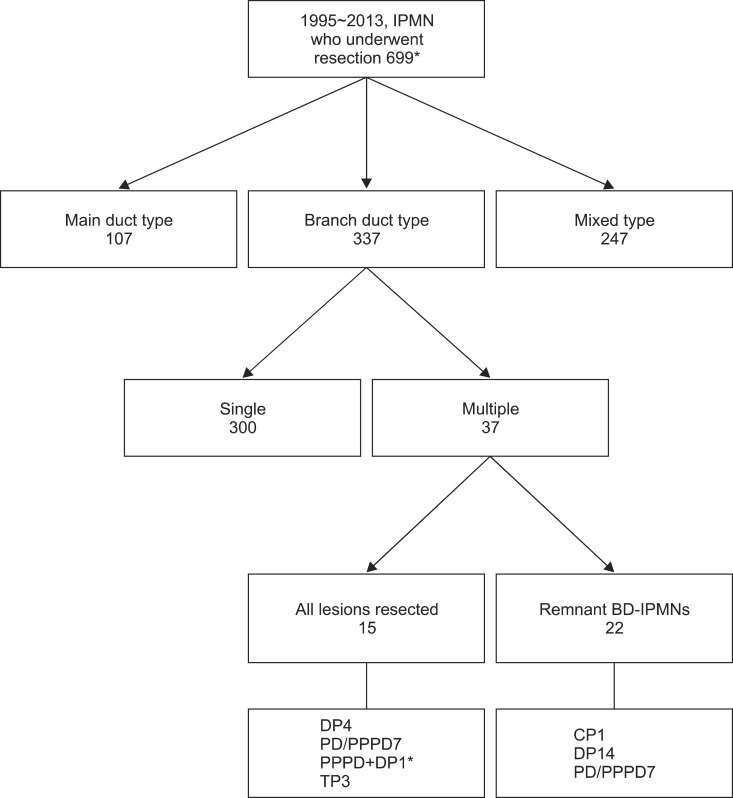 | Fig. 1Flow diagram of 699 patients who received pancreatic resection for IPMNs. DP: distal pancreatectomy; PD: pancreaticoduodenectomy; PPPD: pyloruspreserving. pancreaticoduodenectomy; TP: total pancreatectomy; CP: central pancreatectomy. *Eight patients: unknown ductal type. **PPPD was combined with pancreas tail resection.
|
We defined multifocal BD-IPMNs as two or more cystic lesions in any part of the pancreas that had communication with the main pancreatic duct. Multifocal BD-IPMN was diagnosed using computed tomography (CT) scan or magnetic resonance cholangiopancratography (MRCP) (Fig. 2). MRCP was performed on a 1.5 Tesla MR scanner (Magnetom Avanto, Siemens Medical Solutions) with intravenous injection of Gd-BOPTA (gadobenate dimeglumine, Multihance®). Of the 22 patients, 20 were evaluated by both CT and MRCP. Malignancy of BD-IPMNs was suspected when the followings were observed in preoperative imaging studies: diffused main pancreatic duct dilatation over 10 mm, tumor size over 3 cm, enhanced mural nodules, and lymphadenopathy. Pancreatic resection was performed for all suspicious malignant lesions, whereas benign-looking BD-IPMNs were left intact within the remnant pancreas.
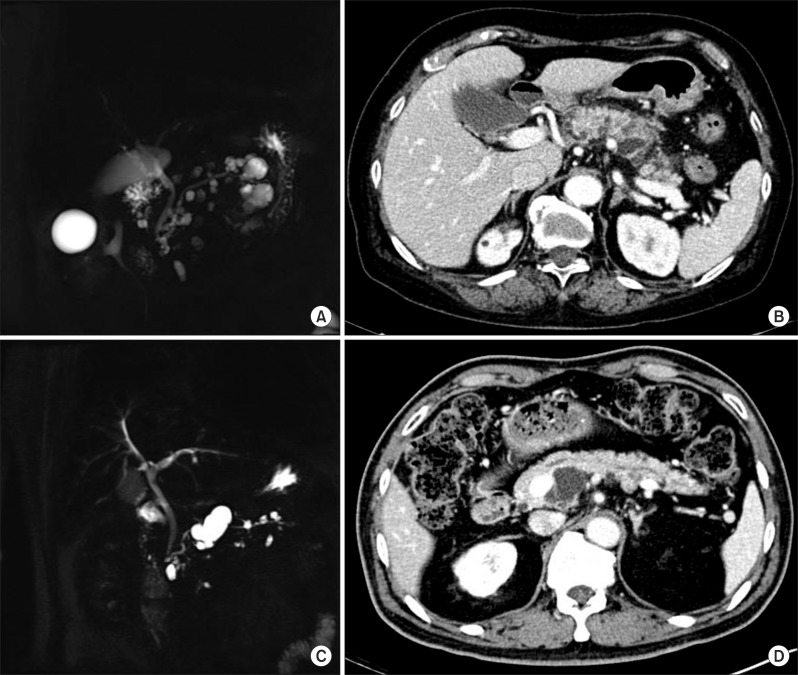 | Fig. 2Radiologic findings of multifocal intraductal papillary mucinous neoplasms. (A and B) MRI and CT scan revealed pancreas swelling with peri-pancreatic infiltration, implying acute pancreatitis. There were variable sized multiple cystic lesions communicated with the main pancreatic duct in the entire pancreas, suggesting multiple BD-IPMNs. Main pancreatic duct size was measured at 3 mm. (C and D) Multifocal BD-IPMNs in the pancreas with maximal diameter measured at 3.5 cm in the uncinate process without evidence of dilatation of main pancreatic duct or mural nodules.
|
Ductal types of IPMNs of resected specimens were classified according to radiologic study and pathologic results. Pathologic classification of resected pancreas was in accordance with World Health Organization classification of tumors.7 Staging system of IPMN carcinoma was based on the latest pancreatic cancer staging system by the American Joint Committee on Cancer (AJCC).8 After operation, patients were followed up by CT scans immediately after the operation (within one month) and at three months, and six months post-operatively. If there was no change in lesions in the remnant pancreas, CT scans with chemical battery and CA 19-9 were performed annually.
Go to :
RESULTS
Clinical and pathological characteristics of the 22 patients (13 males and 9 females, mean age 65 at the time of operation) analyzed in this study are summarized in Table 1. Of the 22 patients, six visited hospital due to abdominal pain or discomfort. Of the six patients, three had pancreatitis. A total of five patients were diagnosed with pancreatitis, of which three had symptom of abdominal pain. Both mean CEA (2.4 ng/ml) and CA 19-9 (7.5 U/ml) were within the normal range (0-6 ng/ml for CEA, and 0-37 U/ml for CA 19-9).
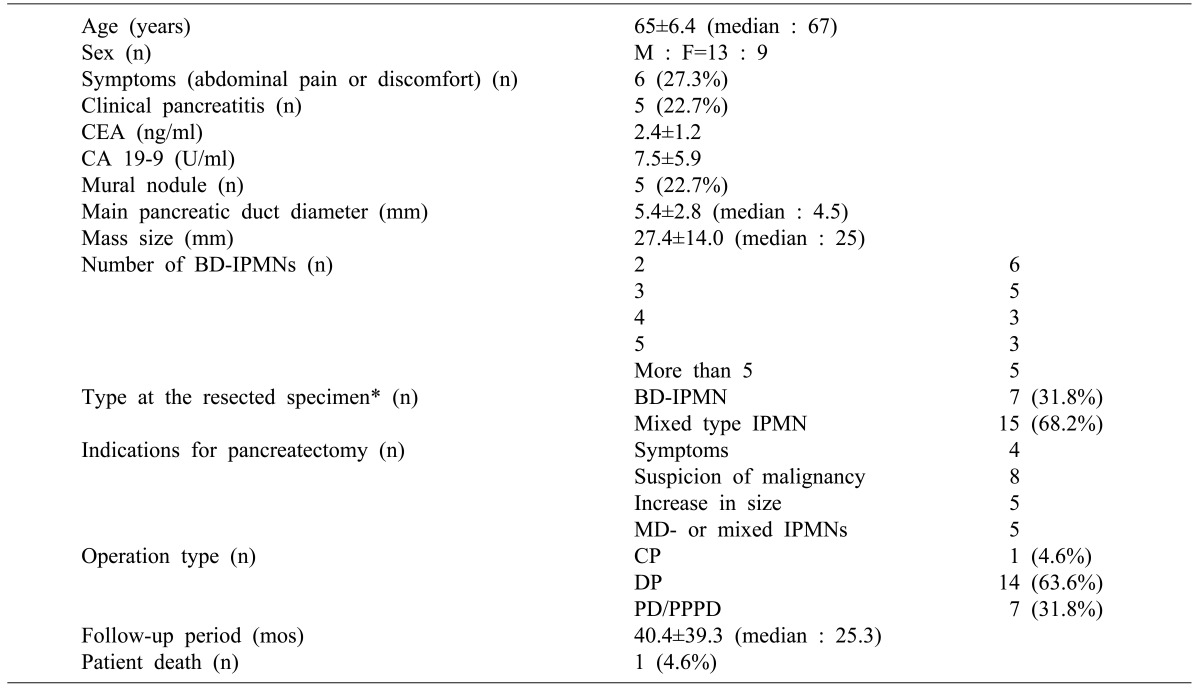
Mural nodules were found in five (22.7%) patients. Mean diameter of the main pancreatic duct was 5.4 mm. Mean diameter of the largest lesion (measured by pathologists) was 27.4 mm. The number of BD-IPMNs evaluated by pathologists or radiologists was: two in 6 patients, three in 5 patients, four in 3 patients, five in 3 patients, and more than five in 5 patients. In 15 patients, IPMNs in the resected pancreas initially assessed as BD-IPMNs by radiologic studies were diagnosed as mixed type pathologically. All 22 patients showed BD-IPMNs in their remnant pancreas revealed by CT or MRCP.
Pancreatic resection was proposed and performed in patients with symptoms of abdominal pain or recurrent pancreatitis (n=4), suspicion of malignancy in radiologic studies (n=8), increase in size during follow-up (n=5), and main duct-IPMN or mixed type IPMN suspected in preoperative radiologic study (n=5). The operation types of pancreatectomy included distal pancreatectomy (n=14), pancreaticoduodenectomy or pylorus-preserving pancreaticoduodenectomy (n=7), and central pancreatectomy (n=1).
Pathologic results of resected pancreas are summarized in Table 2. A total of 17 patients showed low- or intermediate-grade dysplasia. Two patients were diagnosed as high-grade dysplasia. Three patients had IPMN with an associated invasive carcinoma. TNM stage of invasive IPMN carcinomas were IA in one patient and IB in two patients. None of them underwent postoperative adjuvant chemotherapy. Instead, they were observed regularly without evidence of recurrence during follow-up period. All pancreatic resection margins except three patients were negative for tumors. In these three patients, resection margins were IPMN with intermediate-grade dysplasia. Another three patients showed pancreatic intraepithelial lesions 1A (PanIN 1A) in resection margins. One patient had PanIN 1B in resection margin. No perioperative mortality occurred. The mean follow-up period was 40.4 months. During the follow-up, no disease-associated mortality occurred. One patient who had received renal transplantation six years before the pancreatic resection died 35.2 months after the operation. There was no disease progression (no increase in diameter) or recurrence of IPMN in the remnant pancreas during follow-up except in one patient who showed increase in diameters of two remnant BD-IPMNs (from 8.2 mm to 11 mm and from 10 mm to 13.5 mm) 17 months after the pancreatic resection (Fig. 3). Because there was no evidence of malignant features in the remnant lesions, this patient was observed regularly without any intervention. There was no perioperative morbidity. However, one patient showed recurrent pancreatitis after PPPD with pancreatic duct stone. The patient underwent re-operation for pancreaticojejunostomy (PJ) revision 40 months after the first surgery PPPD. After PJ revision, the patient has been doing well without any complication. The remaining twenty patients are now currently alive without any change in follow-up CT scans. No patient had tumor recurrence.
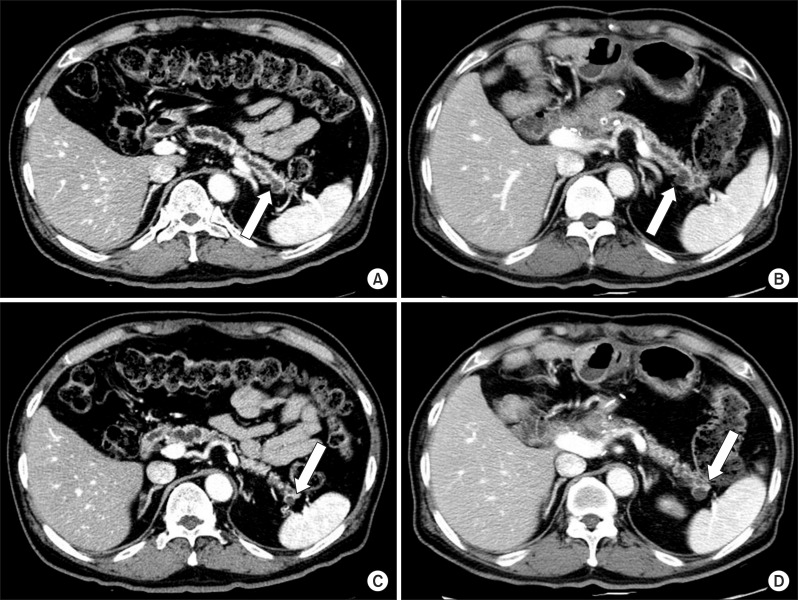 | Fig. 3Patient showing progressive dilatation of BD-IPMN. A 68 years-old male patient underwent pylorus-preserving pancreaticoduodenctomy due to increase in size of multifocal BD-IPMNs with mural nodules in the head. At 17 months after pancreatic resection, follow-up CT scan showed increase in diameter of two remnant BD-IPMNs in the pancreatic tail: (A) from 8.2 mm (B) to 11 mm, (C) from 10 mm (D) to 13.5 mm. Because both of them did not have any high-risk stigmata or worrisome features, we chose to cautiously observe these lesions.
|

Among the 37 patients with multifocal BD-IPMNs, 15 were able to remove all multifocal BD-IPMNs through pancreatectomy. One patient had IPMN with an associated invasive carcinoma. Another patient showed IPMN with high-grade dysplasia. A total of 13 patients had low- or intermediate-grade dysplasia. Indications for pancreatectomy were symptoms of abdominal pain or recurrent pancreatitis (n=3), suspicion of malignancy in radiologic studies (n=7), increase in size during follow-up (n=3), mixed type suspected in preoperative radiologic study (n=1), and patient's desire (n=1). There was no recurrence or disease progression except in one patient who was diagnosed with IPMN associated with invasive carcinoma. Pathologic staging of invasive IPMN was stage IA. The patient didn't receive any adjuvant chemotherapy. Six months after the surgery, the patient was found to have multiple lung metastases on follow-up CT scans which were treated by chemotherapy. The remaining 14 patients have been doing well without any recurrence or progression during the mean follow-up period of 40.4 months.
Total pancreatectomy was performed in three patients, including two patients who had pancreatitis with multifocal IPMNs involving the entire pancreas and one patient who had increase in size and number of IPMNs affecting the entire pancreas. Pathologic results of these three patients were BD-IPMNs with low- or intermediate-grade dysplasia.
Go to :
DISCUSSION
According to the international consensus guidelines for the management of IPMNs,1 surgical resection is recommended for BD-IPMN with 'high-risk stigmata of malignancy' or 'worrisome features' that suggests malignant potential of IPMNs. "High-risk stigmata" include obstructive jaundice, enhanced solid component within cyst, and main pancreatic duct size over 10 mm. "Worrisome features" include pancreatitis, cyst size over 3 cm, thickened or enhanced cyst walls, non-enhanced mural nodules, main pancreatic duct size of 5-9 mm, abrupt change in the main pancreatic duct caliber with distal pancreatic atrophy, and lymphadenopathy. They also advocated surgical resection only for the highest oncological risk even in multifocal BD-IPMN cases using the same treatment strategy as single BD-IPMN. In our study, multifocal BD-IPMNs in remnant pancreas do not have any 'high-risk stigmata' nor 'worrisome features'. They were followed up safely without significant changes in CT scans. Although BD-IPMN itself is bearing the potential to progress into malignancy, if BD-IPMNs do not have any features implying the malignancy, we do not have to remove all BD-IPMNs to avoid the risk of pancreatic insufficiency.
There are several reports on the follow-up of BD-IPMN patients. About 82-97% of BD-IPMNs without mural nodules showed no progression during 42-61 months.9,10,11 Therefore, resection is only indicated for lesions with malignant features. Considering the natural course and the clinical behavior of BD-IPMNs, cautious clinical and radiological follow-up is suggested for asymptomatic small (less than 3 cm in diameter) BD-IPMNs. Similar recommendation could be applied to multifocal BD-IPMNs. Although the natural history and precise prognosis of multifocal BD-IPMNs remain controversial, multifocal BD-IPMNs showed slow growth and non-significant evolution as time elapsed in radiologic follow-up.12 However, Tanno et al.11 suggested that patients with BD-IPMNs had a high risk for metachronous pancreatic ductal adenocarcinoma even though pancreatic cancer developed separately from BDIPMN. Therefore, benign course of multifocal BD-IPMNs should not be overlooked. We need to pay attention to the importance of careful observation and regular follow-up in these patients. In our study, of 37 patients, recurrence developed in only one patient who had all IPMNs in the pancreas removed through PPPD, suggesting that no remnant IPMNs was in the pancreas tail. Recurrence appeared in the form of distant metastasis in the lung 6 months after the pancreatic resection. On the other hand, for all patients who had remnant BD-IPMNs in the remnant pancreas, no recurrence or clinically significant progression of the disease occurred.
In 22 patients with remnant BD-IPMNs in the remaining pancreas, indications for the pancreatic resection were consistent with the 'International Consensus Guidelines 2012' mentioned above, suggesting that BD-IPMNs might have malignant features when CT or MRCP findings show mural nodules, enhancing solid portions, lymphadenopathy, or tumor size over 3 cm.
In this study, we specified our subject to remnant pancreas with multiple BD-IPMNs. Our conclusion is that we can safely preserve pancreas parenchyma with multifocal BD-IPMNs in the remnant pancreas by performing pancreatic resection because they would remain silent without disease progression or recurrence. Regardless of pathologic status of the resected specimen of IPMNs, BD-IPMNs in the remnant pancreas do not affect the survival of patients.
Go to :
 XML Download
XML Download