

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hepatic resection remains the golden standard for treatment of patients with primary and metastatic liver malignancy.1,2 As one of the local ablative techniques available, radiofrequency ablation (RFA) is currently used for treating resectable small hepatocellular carcinoma (HCC).3 Although the effectiveness is less well established, RFA has been widely accepted for treating patients with malignant liver tumors unsuitable for hepatectomy.4,5
Despite its advantages, minimal invasiveness and safety of use, there are some limitations.6 RFA could damage adjacent visceral organs when tumors are located peripherally. Especially, percutaneous RFA can cause pneumothorax or damage to the diaphragm when tumors are located near the dome of the liver. Also, multiple liver lesions limit RFA outcomes.7,8 To overcome these limitations, intraoperative RFA can be used as an alternative.9,10 The use of a laparoscopic or open approach allows placement of RFA electrodes at difficult locations with more accuracy under real time imaging guidance and multiple sites.11 In previous studies, intraoperative RFA was shown to be a safe and effective treatment for HCC in difficult locations.12,13 However, there is a lack of studies comparing the efficacy of both intraoperative methods. This study aims to evaluate the comparative effectiveness of the two intraoperative approaches on the treatment outcomes of RFA for malignant liver tumors.
Go to : 
MATERIALS AND METHODS
From December 2008 to July 2013, we performed intraoperative RFA on 57 patients with malignant liver tumors. The Cool-tip™ (18 Gauge) Radiofrequency Ablation System and the Evident™ Microwave Ablation System (Covidien, CO, USA). were used for RFA procedures. Intraoperative ultrasound examination and radiofrequency electrode insertion into the center of the tumor were performed by an experienced operator. The median time for the radiofrequency current was 12 minutes (range, 10-28 minutes).
Study patients were 39 men and 18 women, with a median age of 65 years (range, 44-86). The median follow up period was 19 months (range, 3-62). Hepatic resection was not recommended for most of the patients based on tumor multifocality. Indications for intraoperative RFA are determined by patient preferences owing to fear of perioperative morbidity and mortality. Difficult locations for percutaneous approach such as the hepatic dome or caudate lobe are also indicated. The operative approach was applied for tumors adjacent to the diaphragm, or in contact with adjacent structures, or when hepatic resection was deemed obligatory, especially in case of bilobar liver metastases where resection and RFA of contralateral tumors should be performed.
Follow-up contrast enhanced computed tomography was performed immediately after surgery and every three to four monthly in the first 2 years thereafter to evaluate the effectiveness of the treatment. Each time patients visited for follow-up, blood tests were conducted including liver function test and serum alpha-fetoprotein (AFP).
All analyses were performed using the statistical software SPSS ver. 18.0 (SPSS Inc., Chicago, IL, USA). Comparisons between the two groups were done using the Student t-test for continuous data and the x2 test for categorical data. The overall and disease-free survivals were calculated using the Kaplan-Meier method. The relative prognostic significance of the variables in predicting overall and disease-free survival was analyzed using multivariate Cox proportional hazards regression analysis. Significant difference was considered when p<0.05.
Go to :
RESULTS
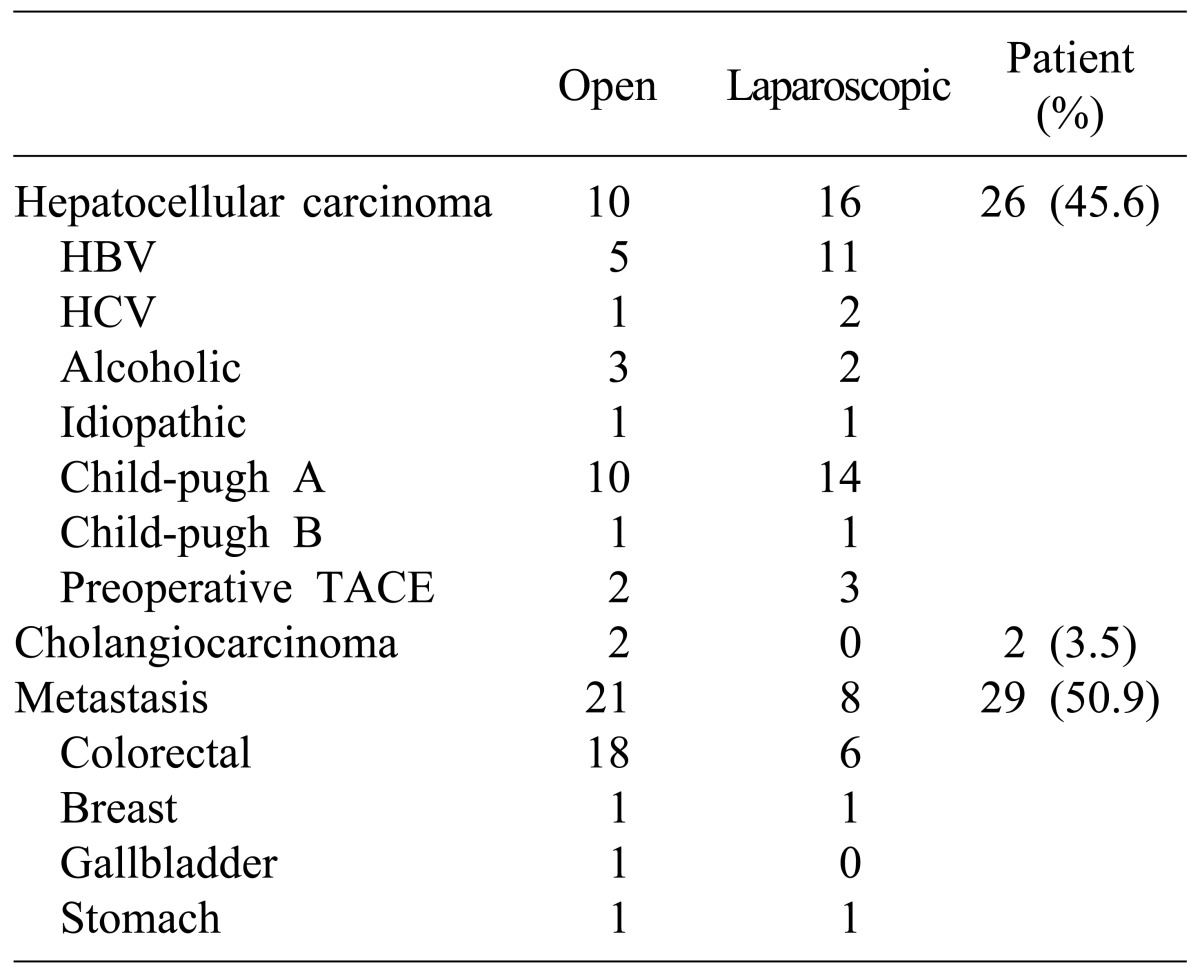
The patient and tumor characteristics are summarized in Tables 1 and 2. There were no significant differences in sex, age, operative method, size of tumor, complication, and whether the tumor location was in the subcapsular region or not. Open surgical RFA was mostly performed at the tumor location of the liver, segment 7 (11 vs. 2, p=0.026). The majority of patients with HCC were Child-Pugh class A (92.3%) (Table 2). The cause of HCC was mainly hepatitis B virus infection (61.5%). Of the 29 patients with metastatic liver tumors, the most common primary malignancy was colorectal cancer (82.8%). Most patients with metastatic hepatic malignancy received open surgical RFA (21 vs. 8, p=0.018). Of 33 patients who underwent open intraoperative RFA, 25 patients received additional surgery simultaneously; liver resection in 19, colectomy in 10, cholecystectomy in 6, gastrectomy in 1, lung resection in 1. The rate of combined operations was significantly different between the open and laparoscopic RFA groups (25 vs. 5, p<0.05).
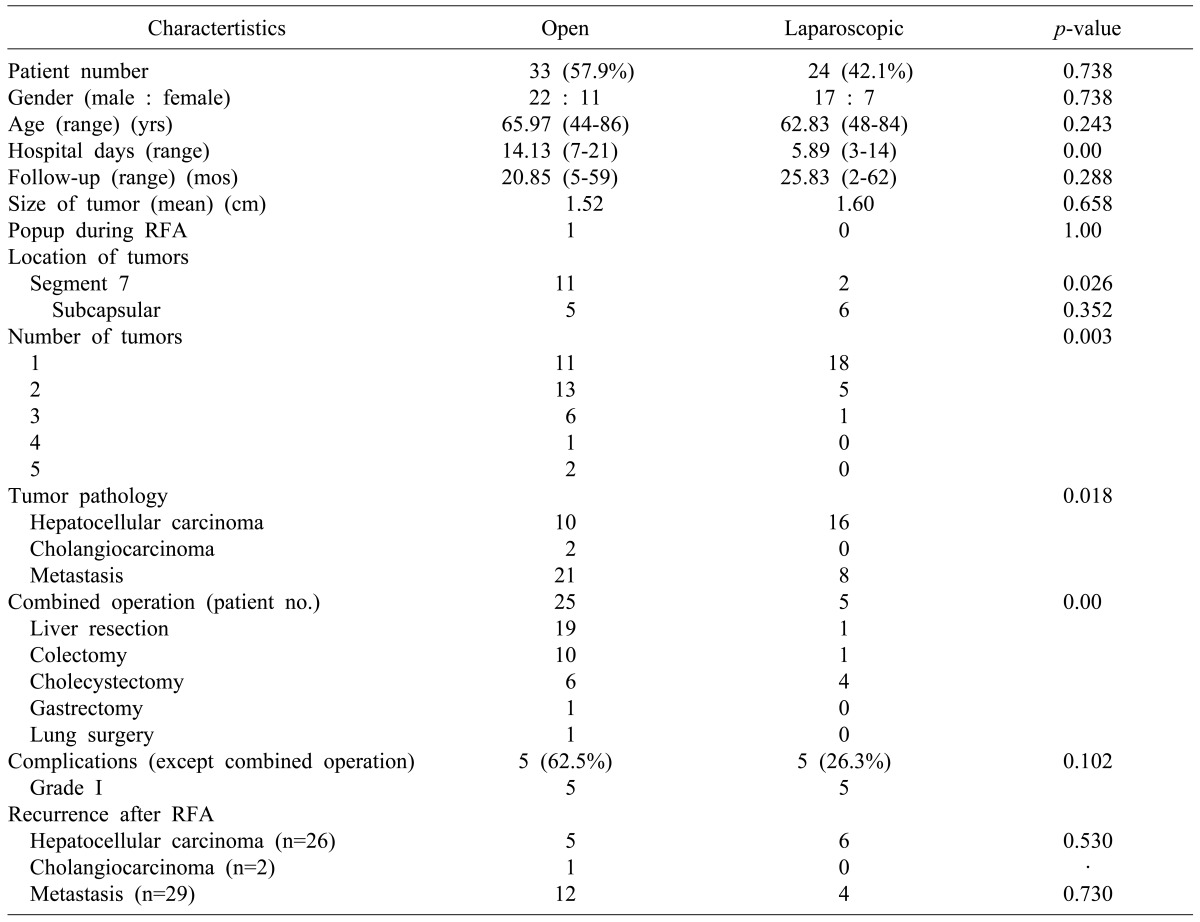
The number of tumors was significantly different between the two intraoperative approaches (p=0.003). However, the sum of multiple RFA sites showed no significant differences (p=0.541). Twenty-three and eighteen patients underwent open and laparoscopic RFA for one lesion, respectively. Seven and five patients respectively received each intraoperative approach for two lesions. Another two and one patients were candidates for the respective surgical methods for three lesions. Only one patient underwent open surgical RFA for 4 lesions.
Hospital stay after surgery differed considerably between the two groups (p<0.05). The median number of days in the hospital was fourteen for open surgical RFA (range, 7-37 days) and 5.5 for laparoscopic RFA (range, from 3-14 days).
All of the complications were classified as grade I, pleural effusion, according to the Clavien-Dindo grading system for classification of surgical complications. Although there were no significant differences between the two groups, the laparoscopic RFA group experienced a lower incidence of complications (62.5% vs. 26.3%, p=0.102).
One patient with HCC (3.8%) showed incomplete ablation on the immediate follow-up computed tomography (CT) scan. None of the patients with HCC showed local tumor progression, but ten had a new lesion (4 for open and 4 for laparoscopic approaches). One of the patients with cholangiocarcinoma had local tumor progression after open surgical RFA but no new lesions. In metastasis cases, two (6.9%) and one (3.4%) patients who underwent open and laparoscopic RFA respectively had local tumor progression whereas ten (34.5%) and three (33.3%) had a new lesion (Tables 3, 4). The median disease-free survival time was 11 months for patients with HCC (range, 2-57 months) and 10 months for those with liver metastasis, especially from colorectal cancer (range, 2-54 months). The difference in local recurrence rates after intraoperative RFA was not statistically significant between the two groups according to the tumor pathology. The overall recurrence rate three-years after open and laparoscopic RFA was 73.3% and 61.4% for patients with HCC (p=0.370), respectively; the rate was 72.2% and 60% for patients with liver metastasis from colorectal cancer, respectively (p=0.354) (Fig. 1).
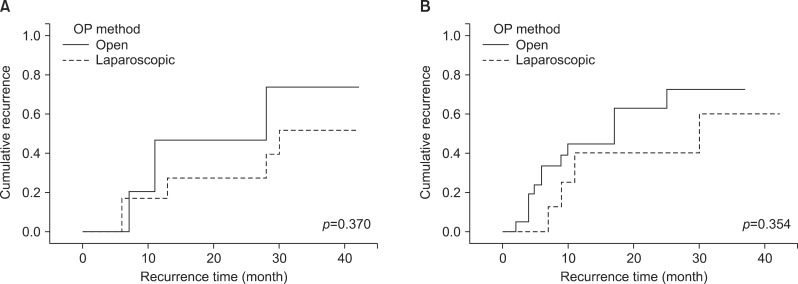 | Fig. 1Comparison of recurrence rates after open and laparoscopic radiofrequency ablation for hepatocellular carcinoma (A) and liver metastasis from colorectal cancer (B).
|


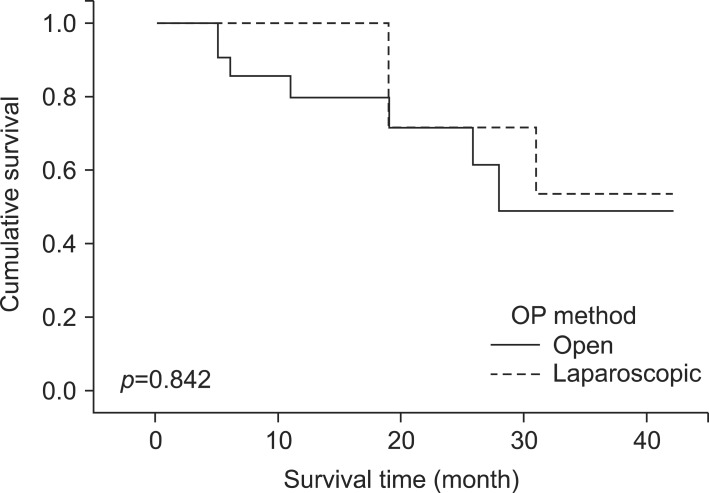
During the follow-up period, there were no mortalities associated with the surgery. One patient each with HCC died of disease progression at thirty and at six months after undergoing open and laparoscopic RFA. The three-year overall survival rates of patients with metastatic tumors from colorectal cancer who underwent open and laparoscopic RFA were 83.7% and 64.0%, respectively (Fig. 2).
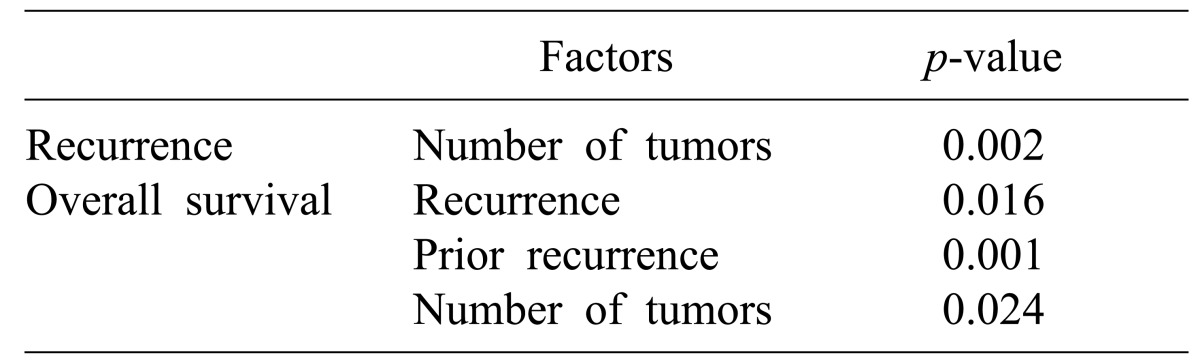
Multivariate analysis was performed to evaluate the effect of factors (e.g., number of tumors, tumor pathology, RFA method, subcapsular location, recurrence case, simultaneously combined operation, Child-Pugh classification, whether complications exist, preoperative chemotherapy and TACE) that may potentially influence the tumor recurrence rate and overall survival (Table 5). The number of tumors was the only significant factor affecting the recurrence rate after intraoperative RFA. Recurrence after RFA, recurred case and number of tumors were independent factors affecting overall survival.
Go to :
DISCUSSION
Radiologists initially used percutaneous RFA as treatment for solid tumors. Surgeons started to use RFA as a surgical approach for patients with tumors at locations that are too difficult for percutaneous treatment.14
Unlike percutaneous treatment, the surgical approach can ablate tumors which are located near major blood vessels or bile ducts and adjacent organs and structures.
Otherwise, for small HCC in locations too difficult to apply a percutaneous approach, intraoperative RFA can be an alternative option for deep-seated tumors.15,16,17
Several studies show that intraoperative RFA (by laparoscopy or laparotomy) results in superior local control compared to percutaneous RFA with similar overall survival and complication rates.18,19,20 To assess the success of RFA treatment, we must closely evaluate the outcome with incomplete treatment, local recurrence, survival rates and complication rates taken into account.21 However, there is no consensus among experts on which surgical approach is more practical.
The rate of incomplete ablation was generally reported to be less than 10% on tumor-by-tumor analysis.22,23,24,25 In our study, there was only one case (1.8%) of incomplete ablation. The patient had HCC in the form of a 1-cm-sized subcapsular lesion located in segment 6 of the liver. Under similar difficult approach conditions in the right posterior segment of the liver (open in 6 and laparoscopic in 7 patients), there was no incomplete treatment in the laparoscopic RFA group.
In a meta-analysis study of local recurrence after hepatic RFA, the total recurrence rate was 14.9% (352 of 2369) for patients with HCC and 14.7% (112 of 763) for patients with colon cancer metastases.19 In that analysis, significantly fewer local recurrences were observed for a surgical (versus percutaneous) approach, (p<0.001) even for small tumors (≤3 cm). In our study, local recurrence rate was 7.0% for all-tumor pathologies. Of the four patients with local recurrence, three received open surgical RFA. Two of the three had liver metastasis and the other had cholangiocarcinoma. There was no local recurrence in patients with HCC in the two groups.
In a study of RFA for 235 patients with colorectal liver metastases, the overall survival rates at 3 years were 20.2%.26 Also, the mean survival for patients with tumors <3 and >3 cm was 28 and 20 months, respectively. It was reported that the overall 3-year survival rates after laparoscopic RFA for 66 patients with HCC were 38%.27 In our study, 3-year survival rates for colorectal liver metastases were 49.4% and 53.6% according to open and laparoscopic operative approaches, respectively (p=0.842). During the follow-up period, the number of deceased HCC patients was two, and each patient died from disease progression at 30 and 6 months after open and laparoscopic ablation. There was no operative mortality in both groups.
A total of 24 (72.7%) and 6 (25%) patients had complications following open and laparoscopic RFA, respectively (p<0.05). The complications were pleural effusion (86.7%), abdominal wall hematoma (3.3%), ascites (3.3%) and fluid collection (6.7%). Almost all complications except two were classified as grade I according to the Clavien-Dindo grading system.27 There was one patient classified as grade III for requiring percutaneous drainage of pleural effusion. The other received blood transfusion, classified as grade II. Both of them underwent open surgical RFA. The higher complication rate of open RFA compared with laparoscopic RFA in this study was related to the combination of operations. Almost two-third of the patients (75.8%) treated with open RFA underwent simultaneous liver resection or colectomy of extra malignant tumors. These complications, especially pleural effusion, are likely related to hepatic mobilization and liver resection. A study reported that combining resection of dominant liver tumors with RFA of the remaining lesions can be expected to increase the complication rate. Even if there was no statistical significance between the two groups when combined operation cases were excluded, the laparoscopic RFA group experienced lower incidence of complications (62.5% vs 26.3%, p=0.102).
In the study of RFA for 231 unresectable hepatic tumors, the median length of hospital stay was 5 days after celiotomy.28 Also, in one of the other studies, after laparoscopic and open RFA, mean hospital stay was 1-3 days and 4-7 days, respectively.29 In our study, except in the case of simultaneous operation, mean hospital stay was 5.0 (3-14 days) and 11.5 days (7-27 days) after laparoscopic and open RFA, respectively (p=0.02).
We think that the intraoperative approach enables accurate access to tumors when the location is superficial or close to adjacent organs. It also permits simultaneous liver or colon resection if necessary. The intraoperative approach allows for detection of additional hepatic or extrahepatic diseases through visualization. Of the two types of RFA approaches, laparoscopic RFA yielded better outcomes in terms of incomplete treatment, local recurrence, complication rates and length of hospital stay. The factors that contribute to positive results after laparoscopic RFA are as follows: because of the upward movement of the diaphragm by pneumoperitoneum, liver movement can be minimal; 12 mmHg pneumoperitoneum causes a 40% decrease of portal vein flow, with a subsequent increase in RFA size; and the minimally invasive approach decreases the morbidity associated with a large incision.30 The laparoscopic approach is used most often for a limited number of tumors, particularly if mobilization of the liver or bowel is necessary, as well as for patients undergoing concomitant laparoscopic liver resection or colorectal resection.
In conclusion, laparoscopic RFA can be performed for malignant liver tumors with lower morbidity rates, less invasiveness and expense compared to an open surgical approach.
Go to :
 XML Download
XML Download