

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Laparoscopic cholecystectomy (LC), the gold standard therapy for cholecystitis, is associated commonly with bile and gallstone spillage during the operative procedure, occurring at a rate of 9 to 40% according to previous reports.1
Reports on the fate of lost stones since the beginning of laparoscopic cholecystectomy in the early nineties mainly asserted the lack of complications from stones in the peritoneal cavity,2-4 but succeeding reports from the mid-nineties on began notifying of the inflammatory complications from intraperitoneally lost stones.5-7 Additionally, reports on the necessity of retrieving the stones or on methods of stone removal are continuing to be made until today.8
Accordingly, we reviewed our cases of stone spillage and loss into the peritoneal cavity during 10 years of laparoscopic experience with reference to the operative situation, characteristics of the stones lost and the long term clinical results.
Go to : 
METHODS
We could trace 47 cases (82.5%) out of a total of 57 patients who had gallbladder stones lost into the peritoneal cavity during laparoscopic cholecystectomy from March 1998 to February 2007, among 575 total patients who received laparoscopic cholecystectomy.
The operation was carried out through the most typical 4 trochar holes, and the resected gallbladder was removed through the umbilical port in the Lap-Bag pouch.
Stone spillage occurred by the stones escaping through a hole in the gallbladder made by cauterization during dissection of the gallbladder from the liver bed, or through a hole made by grasper forceps while the surgeon was grabbing the inflamed friable wall of the body and fundus of the gallbladder.
During forceps holding of the spilled stones for retrieval into the pouch, the stones frequently break down into pieces and are lost. In cases of large stones, stones hide in intraperitoneal folds like the right paracolic gutter, and in the intermesenteric space in the case of small stones. When the stones are muddy, it is especially difficult to retrieve them into the pouch, with fragmentation frequently occurring which leads to massive irrigation being performed to retrieve the stones.
Every effort was tried to remove stones from entering the peritoneal cavity including initial stapling and even suturing of holes in the gallbladder.
From 2003, in the later part of our review, massive irrigation of the peritoneal cavity and pouch using a latex glove finger was used, decreasing the number of lost stones noticeably.
Every patient including one with stones lost into the peritoneal cavity was given antibiotics for 3 postoperative days, and stones lost into the peritoneal cavity were not taken into additional consideration in the postop treatment plan, except for the placement of a negative suction drain for the removal of fragmented stones or the drainage of infected fluid through the right flank port, and explanation about the stones that were lost and the possibility of complications later.
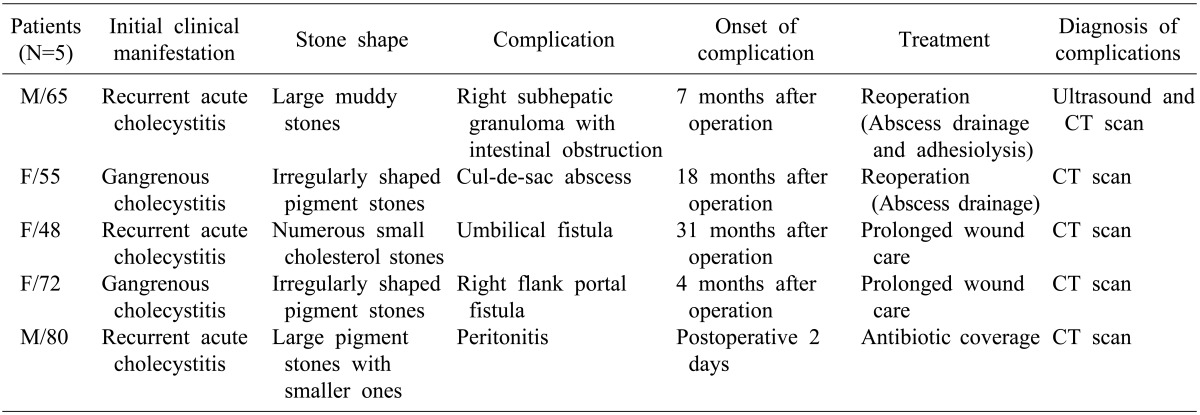
The profile of patients who had complications are shown in Table 1. A descriptive analysis was carried out for statistical analysis.
Go to :
RESULTS
Neither trials of radiologic intervention or surgical procedures were given additionally to patients with lost stones, nor additional admission care or antibiotic coverage.
We experienced 5 cases of complications among patients who had lost gallstones during laparoscopic cholecystectomy. There was 1 case of chronic granulomatous abscess at the right subhepatic space leading to recurrent intestinal obstructive ileus, 1 case of pelvic abscess, 2 cases of fistulous discharge from the umbilical and right flank trochar port respectively, and 1 case of disseminated peritonitis that appeared immediately postoperatively, accounting for a complication rate of 10.6% (5 of 47), which is rather less than the 25% figure quoted by Diez et al.9 and other complication rates in other similar reports.
Above-mentioned complications occurred in a period of time that spanned from the immediate postoperative period (peritonitis with accompanying fever and abdominal distention) to two and half year after the operation (umbilical fistula).
The composition and shape of the spilled stones varied from mucoid or muddy stones to star-shaped pigment stones or round mixed stones. The composition and shape were not related to the complication rate in the stones we have traced.
Intraperitoneal stones evoking abscesses kept their shape when recovered, and stones causing a fistulous tract were finely broken up when being expelled from the body by curettage.
Most cases were diagnosed using CT scan, and treatment was via exploratory laparotomy in 2 cases of intraperitoneal abscess with repeated curettage and wound care at the outpatient clinic for a prolonged time of more than 3 months. One case of peritonitis was treated conservatively with drainage and antibiotic coverage without further complications.
During laparotomy for the 2 cases of intraperitoneal abscess, no further aggressive exploration of the entire peritoneal cavity for hidden stones or for stones that were undetected on preoperative CT scans was attempted. No mortality occurred during the study period.
Go to :
DISCUSSION
Spillage of bile and gallstones during laparoscopic cholecystectomy is very common among surgeons who perform this type of operation, and the incidence is reported to be 10 to 40% of cases.1,9,10
Losing the stones in the peritoneal cavity by the stones hiding in various folds is also a common episode during the operation, and thereby the following reports on this issue are variable in their results. But some reports of serious complications following stone loss, with some recent reports citing complications involving the pleural cavity or major organs11,12 like the liver or kidney, remind us to pay more attention to stones lost in the peritoneal cavity during laparoscopic cholecystectomy.
We reviewed cases of stones lost in the peritoneal cavity in 47 cases, including longterm review and found that there were 5 cases of complications.
Retrieval of stones that have spilled into the peritoneal cavity was not always possible in cases when the stone crumbled when grabbed by forceps into pieces and slid down into folds around the operation field. Once the stones break up, chopping them into smaller pieces for removal by irrigation was attempted but the removal was incomplete. Repeated massive irrigation, using the glove finger pouch since 2003 has helped a lot in removing stones but still some stones are retained.
Some reports recommending mandatory laparotomy or radiological intervention as treatment for retained stones are not favored by most surgeons in view of the fact that unnecessary laparotomies could be performed and considering the approximately 10% inflammatory complication rate.13
Intraperitoneal abscess is one of the serious complications of retained gallstones, requiring interventions such as laparotomy or less likely re-laparoscopy. We did not see this in our cases, but several cases of bowel perforation or internal fistula have been reported with stone retention, probably caused by abscess formation.10
We experienced two cases that were successfully managed by laparotomy. A right subhepatic stone was forming a chronic granulomatous lump with muddy stones in the center and thick walls building around it in its location between the liver and transverse colon. Initially the stones raised the possibility of malignancy causing confusion in the management plan. Jejunal adhesions to the abscess wall were dissected but still adhesive ileus was bothering the patient intermittently. A pelvic abscess with thin walls and containing a pus pocket formed between loops of the small bowel was found and this was successfully irrigated and the small stones were removed. A fistula at the port of the umbilicus and right flank, in our 2 cases, was presumed to be an inflammatory tract originating from an intraperitoneal abscess caused by a foreign body, and drainage was performed through a nearby port. The patients needed wound care and repeated curettage at the outpatient clinic for more than 3 months until fluids ceased to drain. The stones spontaneously exited in fragmented form.
We could not be definitely sure of complete stone removal, since there could be recurrence any time in the future, and other complications like adhesive ileus might arise. Actually in the case above of the patient with a subhepatic abscess, repeated adhesive ileus is still occurring and the patient experiences attacks of vomiting during these episodes. Even after resolution of the complications, nobody knows whether a missed stone will cause complications later, which could impose a continuing threat to the patient's wellbeing.
One positive aspect is that most of the reported complications occurred within several months after laparoscopic cholecystectomy, and in our cases, the latest that complications occurred was two and half years after the operation. And another thing is that, from recent studies in which patients were observed for much longer periods of time, later complications are still occurring until today.14-17
We have not encountered a case of repeated intraperitoneal abscess yet, and have seen no report on these either. But relying on general concepts after a surgical procedure, education should be given without fail to the patient about the persistent risk of various complications that might occur in the area of the operation site or even at other areas where missing stones are located.
We need to be more cautious when dissecting the gallbladder to avoid perforation in any case, especially during dissection along the medial border of the liver fossa where perforation occurred in more than 80% of the perforation cases in our study, and clipping or suturing to prevent stone spillage is still useful, until more advanced instrumentation can better prevent perforation from occurring.
We have to stress that a 10% complication rate is not small by any means, as 42 patients having dormant stones in their peritoneal cavity might be living with the risks of complications of stones in the peritoneal cavity appearing someday in the future. On balance, 10.6% of intraperitoneal lost stones during cholecystectomy caused inflammatory complications including serious ones. Stone are supposed to be removed as far as possible using any method. Surgeons should inform the patient about missing stones and the possible complications that could arise for earlier and easier diagnosis later, just in case. When we find a silent stone during a CT scan that was performed for another reason, we should inform the patient about the stone and possible complications for the same reason.
Go to :
 XML Download
XML Download