

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Intraductal papillary neoplasm of the bile duct (IPNB) or the liver (IPNL) is characterized by a markedly dilated and cystic biliary system and multifocal papillary epithelial lesions.1-3 Frond-like papillary infoldings consisting of columnar epithelial cells with slender fibrovascular stalks are frequently found.2,4 IPNB not infrequently presents with mucin hypersecretion and prominent cysts in the affected bile ducts.5
Chen et al.1 and Nakanuma et al.2 proposed the collective term of IPNB for such biliary papillary tumors after suspecting that IPNB could be a counterpart of IPMN of the pancreas.
Intraluminal papillary tumors of extra- or intra-hepatic bile ducts generally show high or low grade dysplasia or are well-differentiated adenocarcinoma.6-8 These types of tumors are not infrequently associated with superficial spread of carcinoma cells along the biliary mucosa without invasiveness. Approximately 10% of hilar bile duct carcinomas are of the papillary type while approximately 15% of intrahepatic cholangiocarcinoma are intraductal growth type.9 Biliary papillomatosis or papilloma are also sometimes included in this category of biliary tumors.10,11 This type of biliary papillary tumors shows less invasiveness and more favorable outcome compared with other types of intrahepatic cholangiocarcinoma and not infrequently presents as multifocal papillary epithelial lesions in the bile duct with or without mucin production.1-3
Jang et al.12 reported 18 patients who met the definition of IPNB were selected. Five patients showed benign lesions of IPNB, and 13 patients revealed malignant lesions of intraductal papillary adnocarcinoma or cholangiocarcinoma. In 13 patients with the malignant lesions, 1-year, 3-year, and 5-year survival rates were 100%, 84.6%, and 59.2%, respectively.
A case of biliary cystadenoma or carcinoma with ovarian-like stroma was reported. A tumor without ovarian-like stroma was also found in a man patient who showed better prognosis after surgical resection compared to tumors with ovarian-like stroma. Zen and Nakanuma et al. and others examined mucinous expression.2,4,5 The expression of MUC1, MUC2, and CK20 correlated with aggressive from IPNB to invasive or mucinous carcinoma of the bile duct.
We reported intrahepatic and extrahepatic intraductal papillary mucinous adenoma of the bile duct that were completely resected.
Go to : 
CASES
Case 1
A 69-year-old woman was admitted to the hospital with a fever and abdominal pain for several days. Biochemical tests were unremarkable. Ultrasound examination revealed on 3.5×2.5 cm sized mass like lesion at extrahepatic proximal bile duct. Computed tomography demonstrated a 3.5×2.5 cm sized rounded soft tissue mass in the proximal common hepatic duct (CHD) and dilated bile ducts (Fig. 1). MRI showed 2.6 cm by 3.9 cm sized signal void lesion in the proximal common duct and the dilatations in both IHDs (Fig. 2). Preoperative diagnosis was a Klatskin's tumor. We underwent common bile duct resection with hepaticojejunostomy. The proximal CHD mass was polypoid firm mass (3.5×2.5×2 cm). Gross histologic finding showed solid and grayish white mass with focal necrosis in the proximal bile duct. A microscopic view of papillary growing neoplams composed of elongated villotubular structure of epithelial cells with extracellular mucin production (Fig. 3). We confirmed intraductal papillary mucinous adenoma, exrtrahepatic type. The post-operative course was unremarkable, and the patient was discharged on the 10th day post-surgery.
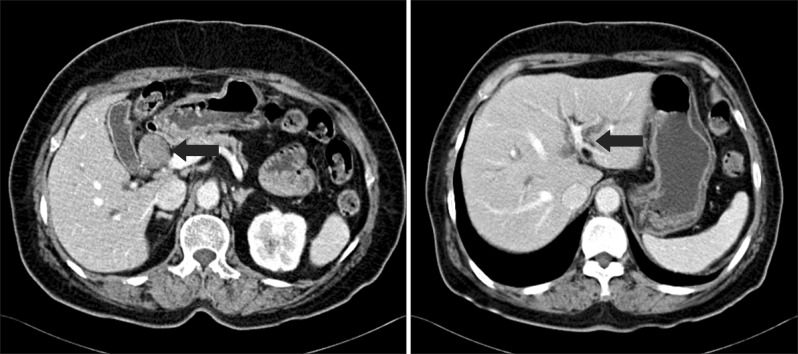 | Fig. 1Contrast-enhanced CT showing a 3.5×2.5 cm sized rounded soft tissue mass (black arrow) in the proximal common hepatic duct (CHD) and dilated bile ducts (black arrow).
|
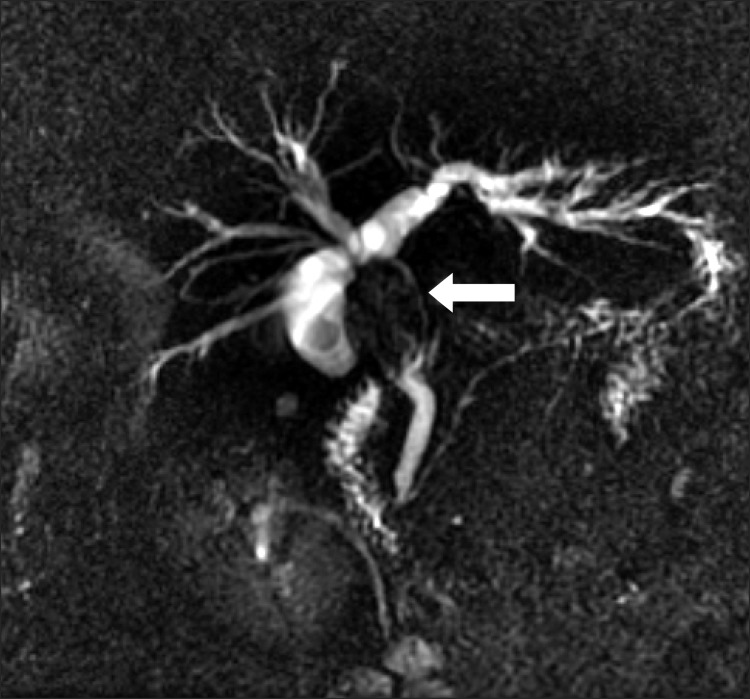 | Fig. 2MRI showing 2.6 cm by 3.9 cm sized signal void lesion in the proximal common duct and the dilatations in both IHDs (white arrow).
|
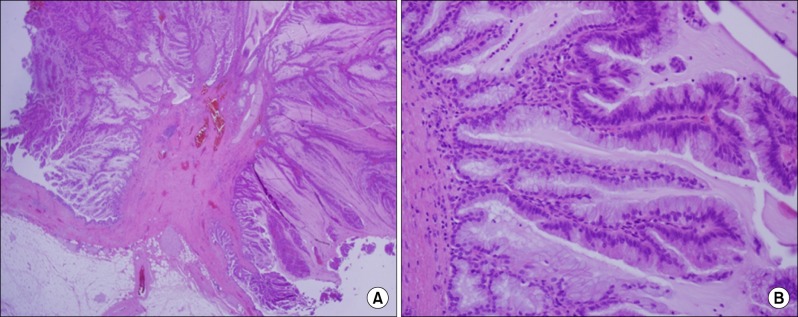 | Fig. 3A microscopic view of papillary growing neoplasm of proximal bile duct composed of elongated villotubulor structure of epithelial cells with extracellular mucin production. (A) H&E, ×40, villotubulor structure of epitherial cells; (B) H&E, ×200, multiple ductules with tall columnar mucinous epithelial cells.
|
Case 2
A 77-year-old woman was admitted to the hospital with discomfort of upper abdomen. Biochemical tests were unremarkable. Ultrasound examination revealed on 7.5×6 cm sized complex cystic mass with internal solid portion in left lateral segment of liver (Fig. 4). Computed tomography demonstrated a well-defined 7.5×6 cm sized cystic mass with internal debris in the left lateral segment of liver (Fig. 4). Preoperative diagnosis was a intrahepatic cholangiocarcinoma. We underwent Lt. lateral segmentectomy of the liver. Gross histologic finding showed an encapsulated multilobular cystic mass (7.5×6 cm), filled with clear mucinous fluid (Fig. 5A). The inner surface of cyst showed multifocal papillary projections. Papillary epithelial mass lined by relatively well-oriented columnar shaped epithelial cells with mild nuclear atypism. The cystic wall lined by single layer of mucous cells supported by loose fibrosis without ovarian stroma (Fig. 5B). We confirmed a intraductal papillary mucinous adenoma, intrahepatic type. The postoperative course has been uneventful to date.
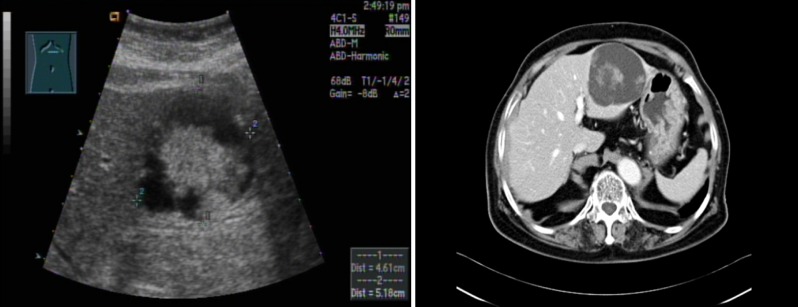 | Fig. 4Ultrasound examination showing 7.5×6 cm sized complex cystic mass in left lateral segment of liver with internal solid portion. Contrast-enhanced CT showing a well-defined 7.5×6 cm sized cystic mass with internal debris in the left lateral segment of liver.
|
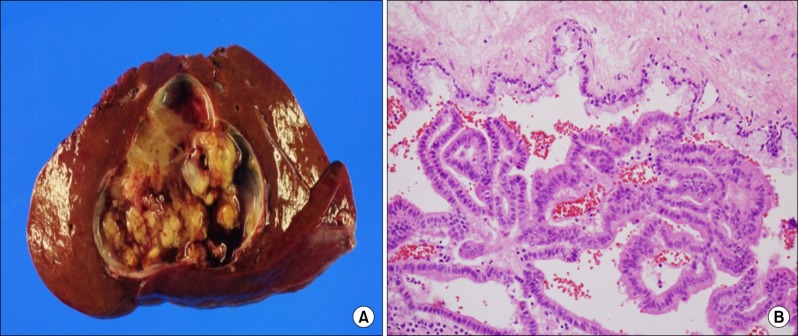 | Fig. 5A gross (A) and microscopic (B) view of papillary growing intraluminal mass. (A) An encapsulated multilobular cystic mass, filled with clear mucinous fluid. The inner surface of cyst shows multifocal papillary projections. The cut surface of the lesion is heterogeneously solid, yellowish tan and granular. (B) H&E, ×200, Papillary epithelial mass lined by relatively well-oriented columnar shaped epithelial cells with mild nuclear atypism. The cystic wall lined by single layer of mucous cells supported by loose fibrosis without ovarian stroma.
|
Go to :
DISCUSSION
Intraductal papillary neoplasm of the bile duct (IPNB) is a new entity proposed by Zen et al. in 2006.5,13 There has been an increase in the number of reported cases of biliary neoplasms of the hepatobiliary system characterized by marked dilatation of the bile ducts or cystic biliary lesions with or without mucin secretion, and mucinous lesions or tumors, possibly due to recent advances in radiological diagnosis.14-18 The number of patients who undergo surgical treatment for such lesions has also increased due to diagnostic and surgical improvements along with development of imaging modalities.4,19 To date, such tumors have been diagnosed and treated under different pathological diagnoses. Nakanuma et al. recently proposed that such tumors could be collectively termed IPNB with the concept that IPNB may evolve through a common pathologic process and shares clinicopathological features with pancreatic IPMN.2 Helical CT and MR imaging can identify dilatation and cystic changes in the biliary and pancreatic ducts in asymptomatic patients.15-17 Enabling diagnosis of malignancy possible and providing reliable follow-up of the patients. Mucobilia detected as a filling defect by cholangiography is characteristic for diagnosis of IPNB.4,14,17,18,20 It should be necessary to consider IPNB in patients showing dilated bile duct without mucin production as well. In my cases, the first patient was old and had symptoms with fever and chilling sense, it might be able to check a ultrasound of liver. That image was helpful to diagnose a disease. The second patient was also older and had a vague discomfort of abdomen with distended epigastrium. Check-up by image diagnosis is necessary in old patients with such complaints. I could not check ERCP for confirming mucin secretion because patients denied.
Although CEA or CA19-9 are usually elevated in biliary malignancies.21 Levels of these tumor markers were within normal range in my cases, and therefore these markers may not be sensitive diagnostic tools for early-stage IPNB. Yeh et al. reported that elevated serum CEA level was helpful in distinguishing intraductal growth type of intrahepatic cholangiocarcinoma and intraductal papillary neoplasm of the liver (=IPNB) as a precursor lesion.
Devaney and colleagues summarized the clinical features of hepatobiliary cystadenomas and cystadenocarcinomas.22 Ovarian-like mesenchymal stromata was detected in 85% of their patients. A tumor without ovarian-like stroma was also found in a man patient who showed better prognosis after surgical resection compared to tumors with ovarian-like stroma. Therefore, IPNB might be included their series. My two cases did not show ovarian-like mesenchymal stroma in the sub-epithelial stroma. Understanding the histopathological findings of IPNB would be useful for intraoperative diagnosis, which may contribute to complete surgical resection and better patient prognosis. IPNB or intraductal papillary growth type of intrahepatic cholangiocarcinoma is a good indication for surgical resection, and complete resection is associated with better prognosis compared with other cholangiocarcinomas.23-25 Therefore, to accomplish good prognosis after treatment for IPNB, diagnosis at the earliest stage followed by curative resection is necessary.
In conclusion, we reported two patients outcome after surgical resection. The latest image diagnostic tools were useful to find and diagnose IPNB. Since the malignant potential of IPNB is lower than other intrahepatic cholangiocarcinoma or bile duct carcinoma, surgical resection is a better therapeutic choice for IPNB.
Go to :
 XML Download
XML Download