

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Peribiliary cysts originate from cystic dilatation of the peribiliary glands.1 Almost all the peribiliary cysts are found in patients with advanced liver diseases, and particularly with disturbance of the portal venous systems, as almost all patients have severe portal hypertensions.
Peribilary cysts should be distinguished from premalignant conditions, such as Caroli's diseases, localized primary sclerosing cholangitis, mucinous cystic neoplasm (MCN) and intraductal papillary neoplasm of the bile duct (IPNB).
Surgical treatment was indicated for our patient, as the diagnosis of Caroli's disease could not be excluded in the present case of a young patient. Subsequently, he underwent elective liver resection. Herein, we report a case of peribiliary cyst resembling unilobar Caroli's disease for a healthy young patient.
CASE
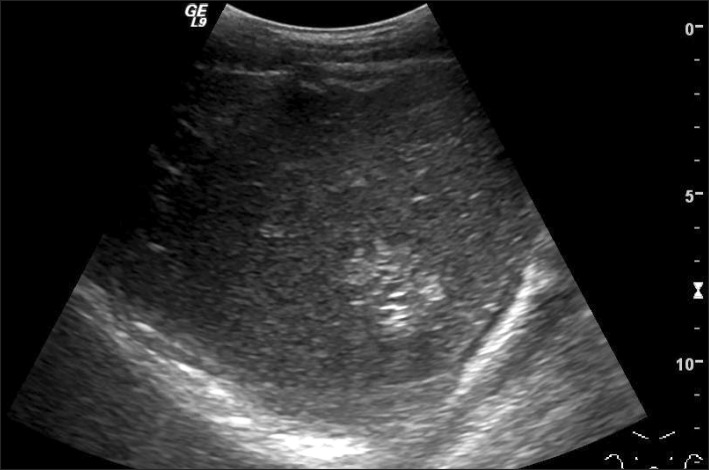
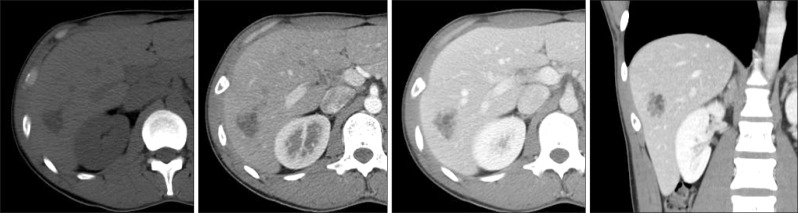
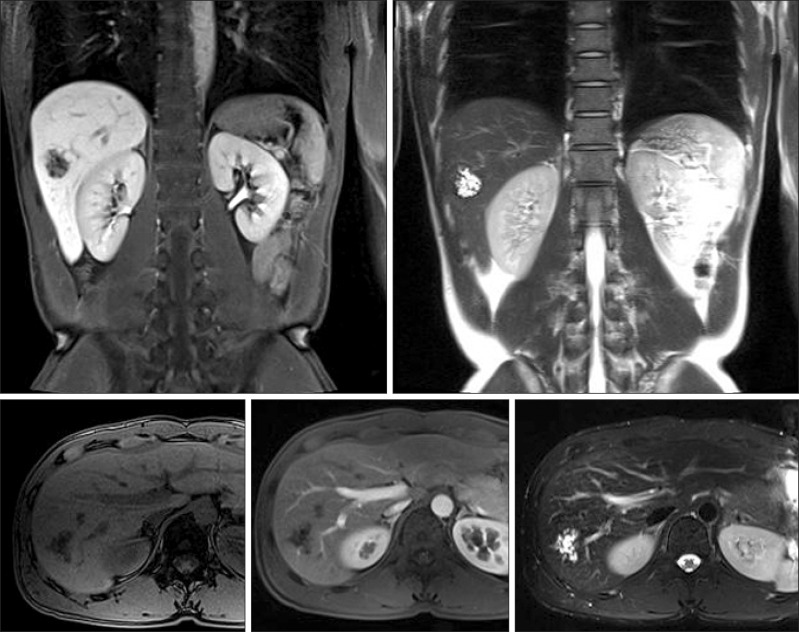
A 31-year-old man was referred to our hospital for further evaluations on the presence of hepatic mass, detected by ultrasonogram (US) performed for routine screening examinations (Fig. 1). The patient was asymptomatic. He had no history of liver diseases or alcohol abuses. All the routine laboratory tests, including liver function tests and tests for tumor markers, yielded normal findings. An ultrasonogram indicated a 3 cm sized multiseptated cystic mass in the right hepatic lobe. An abdominal computed tomography (CT) scan and a magnetic resonance cholangiopancreatography (MRCP) demonstrated a 2.8×2.2 cm sized multilocular, irregular cystic mass in segment VI (Fig. 2, 3). The mass was located at a distance from the hepatic hilum. The findings suggested unilobar Caroli's disease or biliary cystic neoplasm, such as mucinous cystic neoplasm or intraductal papillary neoplasm of the bile duct. Regarding the potential risk of malignancy in the context for suspected Caroli's disease, the mucinous cystic neoplasm and intraductal papillary neoplasm of the bile duct were discussed with the patient, who consequently opted for surgical resection.
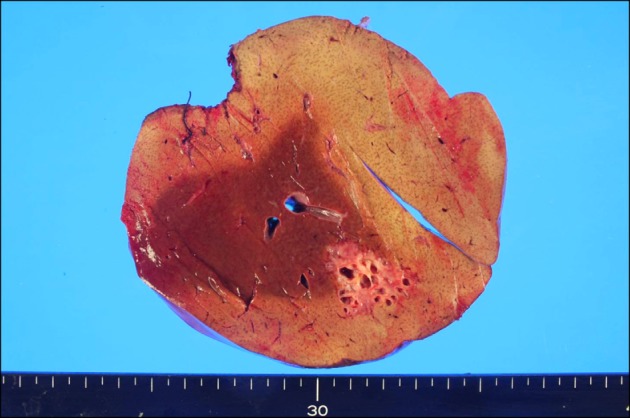
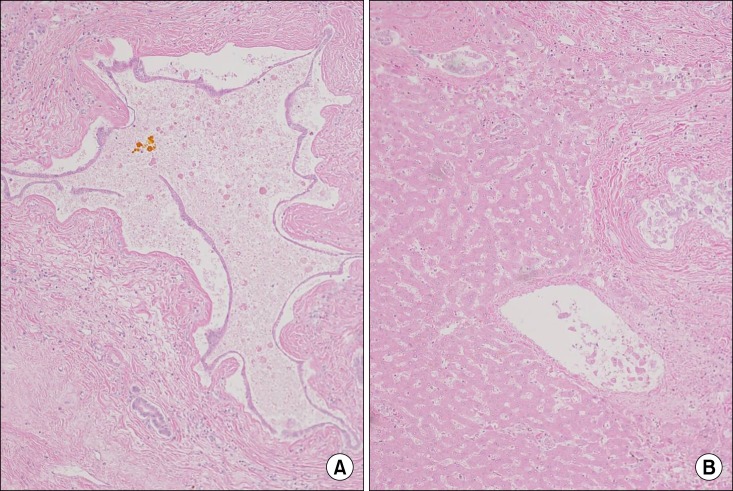
A right hemihepatectomy was performed. At laparotomy, multiple cystic lesions were found surrounding the segment VI bile duct. The patient was discharged 2 weeks following surgery without any complications. Histological examinations of the resected specimen showed multiple cysts distributed along the major segmental portal tracts of the segment VI (Fig. 4). On microscopic examination, numerous peribiliary cysts lined by cubic or flattened epithelium were seen around normal intrahepatic bile ducts. There was no evidence of dysplasia (Fig. 5).
DISCUSSION
Peribiliary cysts were first described by Nakanuma et al. in 1984, as an incidental finding in seven autopsy livers.1 The authors suggested that the peribiliary cysts arose from cystic dilatation of the intrahepatic extramural peribiliary glands in the periductal connective tissues. Terada and Nakanuma have reported the presence of peribiliary cysts in 202 livers (20.2%) among 1,000 consecutive autopsy livers.2 However, the degree of cystic dilatation varies, and the majority are microscopically recognized. In clinical practices, the conditions are still poorly identified.
Until today, the pathogenesis of peribiliary cysts is unclear. Inflammation and circulatory disturbance in the liver are considered as possible mechanisms of cystic formation because the cysts are mainly found in patients with severe liver diseases, such as liver cirrhosis, alcoholic liver diseases, portal hypertensions, or thrombosis.1-4 Genetic predisposition may exist as peribiliary cysts have been reported in association with autosomal dominant polycystic kidney diseases.5 However, in our case, peribiliary cysts were developed without any underlying hepatic diseases. This observation supports a developmental etiology. Fusai et al. have reported the development of peribiliary cysts in normal underlying livers.6
Peribiliary cysts are usually asymptomatic. In some patients, they often increase in size and number, resulting in obstructive jaundice.7,8 However, peribiliary cysts are commonly known as being harmless. Until today and to the best of our knowledge, no cases of malignant degeneration have been documented so far. Once peribiliary cysts are diagnosed accurately, the hepatectomy is unnecessary and follow-ups without invasive treatments are recommended. In our case, preoperatively, the cystic lesion was considered as a unilobar Caroli's disease. Caroli's disease is associated with cholangiocarcinoma. Cholangiocarcionma has been reported in approximately 7% of patients with Caroli's diseases.9 Consequently, hepatectomy was being performed in our patient.
Upon imaging, peribiliary cysts may sometimes be mistaken for biliary dilatations, especially on US examination. Drip infusion cholangiographic (DIC) CT is useful for diagnosis of peribiliary cysts.10 In diagnosing peribiliary cysts, the most important factor demonstrates that the cysts have no communication with the biliary tract. On DIC-CT, peribiliary cysts are not filled with contrast materials since these cysts do not communicate with the lumen of the biliary tree. MRCP is also useful in the diagnosis of peribiliary cysts. Biliary dilatations are demonstrated as tubular structures on one side along the portal tracts. On the other hand, peribiliary cysts usually exist on both sides along the portal tract, which is diagnostic. Nevertheless, in some cases, distinguishing peribiliary cysts from biliary dilatations is a difficult task.
Histologically, the cyst epithelium is cuboidal or of low columnar, thus, is relatively poor in mucus and rarely shows papillary proliferative features.2 In literature, there are no reported cases of malignant transformations.
Peribilary cysts can occur in the normal liver and can mimic the conditions of unilobar Caroli's disease. Accurate identifications of peribiliary cysts and differentiations from other potentially premalignant or malignant cystic lesions are mandatory.
 XML Download
XML Download