

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
With the prolongation of average life expectancy, the incidence of high risk surgery such as a pancreaticoduodenectomy (PD) in old age patients, who have usually been defined in the literature as patients over 70 years old,123 is increasing. Due to advances in surgical and anesthetic techniques, operative mortality in elderly patients has declined over the past few decades.4 Nowadays, an increasing amount of evidence shows that age alone is not an adverse factor in surgery.56 However, although mortality associated with PD has decreased dramatically to less than 5% over the past two decades in high-volume centers, 789101112 the postoperative morbidity rate has remained stationary. Therefore, for some elderly patients with resectable distal common bile duct (CBD) cancer, some surgeons have hesitated to perform curative resection because of the prejudice that the patient might be more likely to have complications due to old age and a poor prognosis from the disease itself. Considering that complete surgical resection of bile duct cancer offers a chance for a cure and long-term survival,131415 evidence whether old age negatively affects outcomes of patients who undergo PD is unclear.
We have analyzed surgical results and survival, comparing two groups (age ≥70 versus age <70) that underwent PD for the treatment of distal CBD cancer.
Go to : 
METHODS
Study population and study design
Between January 2003 and December 2009, 163 patients underwent surgery - PD with curative intent - for bile duct cancer at Keimyung University Dong San Medical Center. For 55 of them, PD including pylorus-preserving PD (PPPD) was performed for treatment of distal CBD cancer, and these patients were enrolled in our study. These patients were divided into two groups according to their age: a younger group (age less than 70 years old) and an older group (age 70 or greater).
Perioperative management and operative procedures
There were no absolute criteria for performing preoperative biliary drainage. In general, if the patients showed jaundice and a bilirubin level higher than 7-10 mg/dl, or if it was necessary to do a biopsy, biliary drainage was applied. Biliary drainage was done by endoscopic retrograde biliary drainage, endoscopic nasobiliary drainage or percutaneous transhepatic biliary drainage. Preoperative diagnosis was done based on computed tomography and magnetic resonance cholangiopancreatography or cholangiography. PD was performed when the level of bilirubin was decreased down to 5 mg/dl.
The PD procedure consisted of standard PD or PPPD, including regional lymph node dissection around the porta hepatis, retropancreatic and celiac trunk area and paraaortic lymph node if necessary. In most cases, PPPD was performed and when the tumor was suspected to be advanced locally, especially in the first portion of the duodenum or distal stomach, PD was performed. The reconstruction of the pancreas was done by the Dunkin method or by a duct-to-mucosa technique. In the Dunkin method, a polyethylene tube was inserted into the pancreatic duct and brought out externally via a transhepatic route in order to drain of the pancreatic juice externally for 2-3 weeks.16 In the duct-to-mucosa method, an internal stent was inserted into the pancreatic duct when the diameter of the pancreatic duct was less than 4 mm, but not if the diameter of the pancreatic duct was larger than 4 mm, stent.
Analysis of perioperative results
Collected data included demographics (sex, tumor marker, tumor size, preoperative bilirubin level, the stage of the cancer (AJCC 7th), tumor differentiation, perineural invasion, lymphovascular invasion, and lymph node metastasis), surgical results (surgical procedure, duration of the operation, amount of bleeding, intraoperative transfusion and curability, morbidity) and hospital stay length. Outcomes of the two groups were compared for perioperative morbidity, mortality and survival rates. Postoperative surgical complications, including pancreatic fistula and delayed gastric emptying, were defined and graded, as described by the proposed Clavien classification system17: grade I as any deviation from the normal postoperative course without clinical significance, grade II as requiring pharmacological treatment, grade III as requiring surgical, endoscopic or radiological intervention, grade IV as life-threatening complications requiring intermediate or intensive care unit management, and grade V as death of a patient. Furthermore, pancreatic fistula was defined according to the International Study Group of Pancreatic Fistula (ISGPF) classification scheme (grade A, B, C)18 and the grade of delayed gastric empting was defined according to the International Study Group of Pancreatic Surgery (ISGPS)19 classification scheme (grades A, B, C). Surgical mortality was defined as death noted within 30 days postoperatively.
Postoperative follow up of patients
All patients were monitored at 3-6 month intervals by measuring levels of CA 19-9, CEA and performing a CT scan annually for the first 2 years and then at 6-12 months interval.
Statistical analysis
Numeric variables were expressed by mean and standard deviation. Patients' demographics and surgical results were evaluated using the chi-square test and Mann-Whitney test, using SPSS for Windows version 18.0 (SPSS Inc., Chicago, Illinois). Survival analysis was done using the Kaplan-Meier method. Differences in survival between groups were compared using the log-rank test. Significance was accepted when the probability was less than 0.05.
Go to :
RESULTS
Clinicopathologic findings
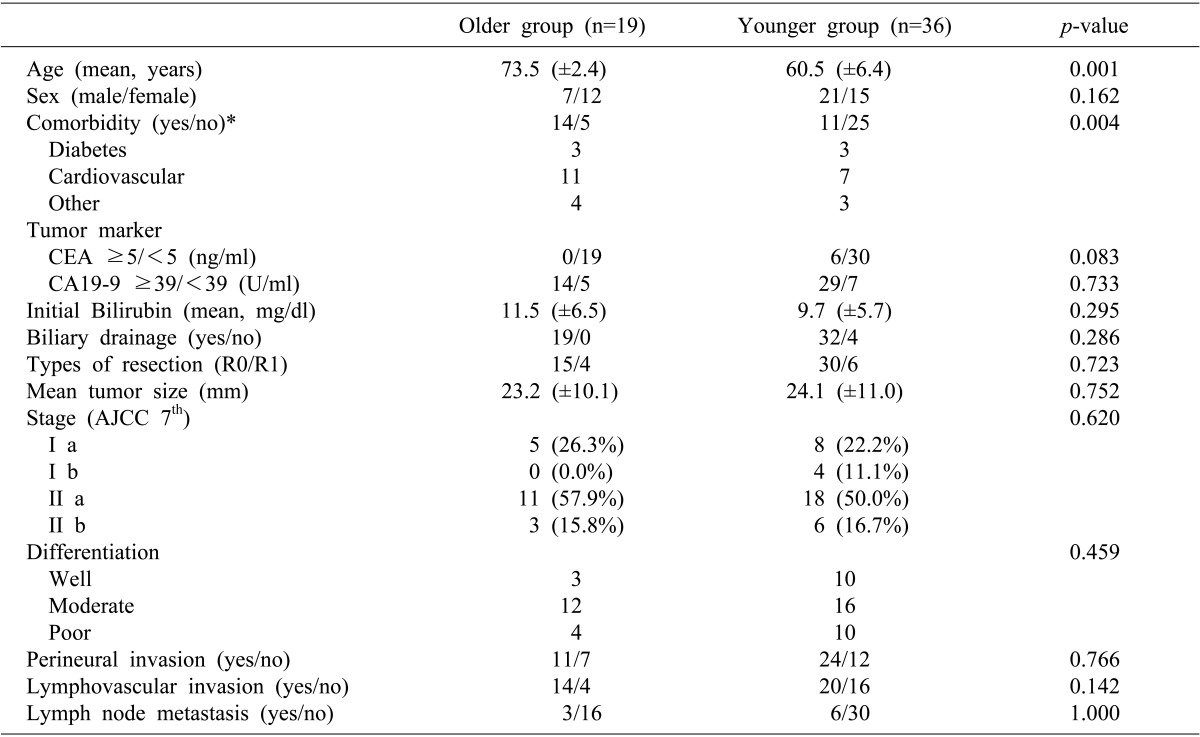
Characteristic of the 55 patients are summarized in Table 1. Of the 55 patients having curative resections, 19(34.5%) were in the older group and the remaining 36 patients (65.5%) were in the younger group. The mean ages of the two groups of patients were 73.5±2.4 years and 60.5±6.4 years respectively. The older patients had significantly more comorbid diseases such as diabetes and cardiovascular disease. Demographic factors and clinicopathologic findings were similar in the two groups.
Perioperative outcomes
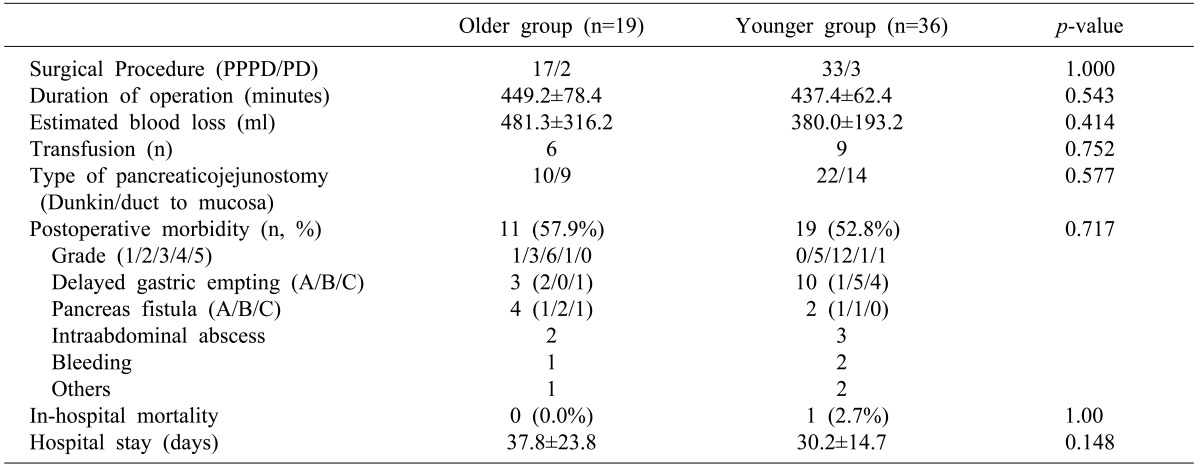
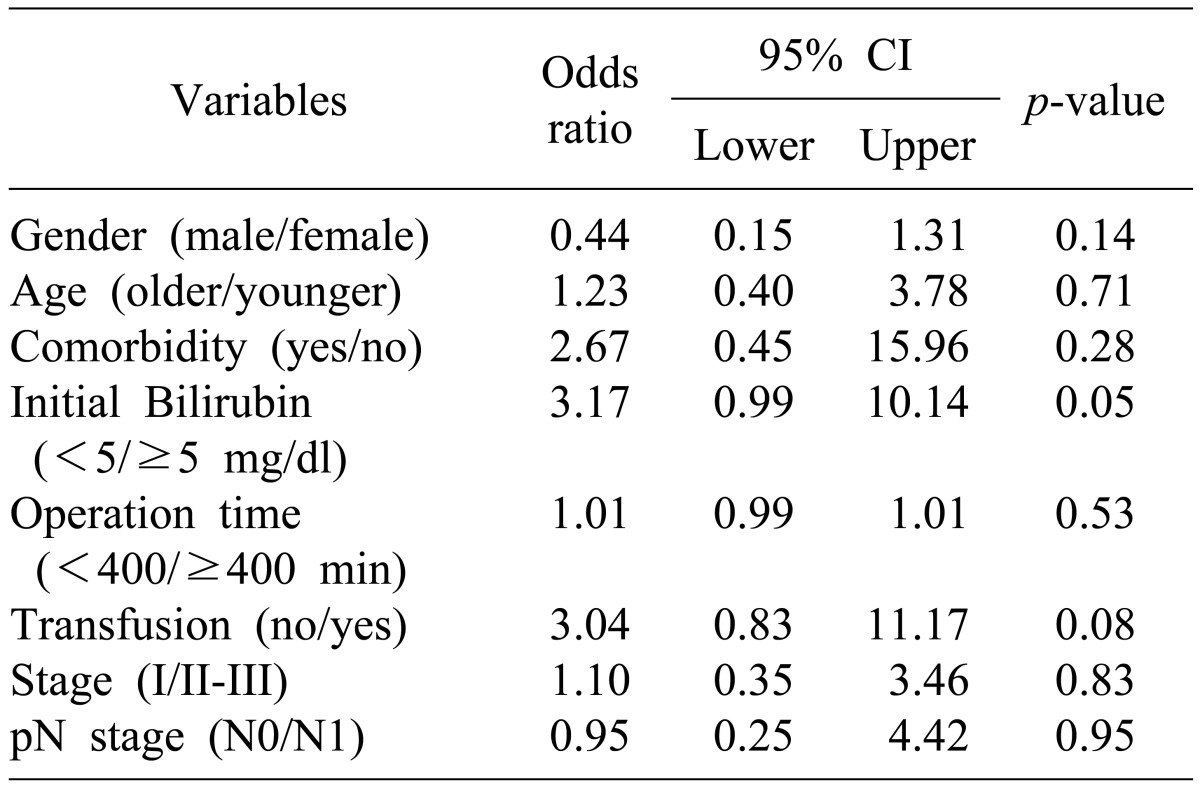
Postoperative short-term outcomes are shown in Table 2. There were no significant differences between the groups in terms of operation time, estimated amount of intraoperative bleeding and duration of postoperative hospital stays. There was no significant difference in the postoperative surgical complication rate (57.9% in Older group Vs 52.8% in Young group, p=0.717) and grade of complication according to the Clavien classification. One patient of the younger group was dead on the 3rd postoperative day due to myocardial infarction. A higher level (more than 5 mg/dl) of preoperative initial bilirubin showed significant correlations with operative morbidity by univariate analysis and age was not an independent risk factor of operative morbidity (Table 3). However, no factors were significantly correlated with operative morbidity by multivariate analysis.
Patient survival
During a mean follow-up period of 34.4 months, the 5-year survival rate was analyzed in the two groups. Overall 5 year survival of the older and younger groups were 45.9% and 39.5% respectively (p=0.671) and disease free 5 year survival rates were 31.7% and 31.1% respectively (p=0.942). There were no significant differences between the two groups (Fig. 1).
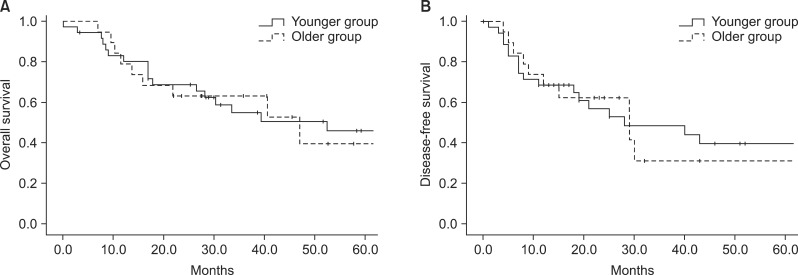 | Fig. 1Comparison of survival according to age group. (A) Cumulative overall survival in Older and Younger groups; the difference between the two groups was not statistically significant (p=0.671). (B) Cumulative disease-free survival in the two groups; the difference between the two groups was not statistically significant (p=0.942).
|
Go to :
DISCUSSION
The elderly population has been increasing progressively as a result of the increased life expectancy worldwide. The average life span of Koreans is currently 74.4 years for men and 81.8 years for women. In 2020, the percentage of the population aged 65 and older in Korea is projected to exceed 20%.20 With the rapid growth of this population, surgeons now face the challenge of providing care for the elderly population. Therefore, it will become more important for surgeons to identify the factors that affect the outcomes of surgery.
Elderly patients have a greater frequency of comorbidity than younger patients do. These disorders include cardiovascular disease, diabetes, respiratory disease and liver disease. These factors may affect recovery from high risk surgery.21 It was reported that an age older than 70 years was an independent predictive factor of postoperative mortality after colorectal surgery.22 However, several recent studies have shown that various operation in the elderly are safe, and that old age alone should not be a contraindication to surgery.232425 Accompanying illness and an advanced stage of tumor, prolonged operation times and excessive blood loss had close relationships with postoperative complications in elderly patients.2526 In particular, preoperative comorbidities have been reported to significantly increase postoperative complications, and it might be possible that elderly patients who have comorbidities are more vulnerable to morbidity or mortality than younger patients.
Our results show that a high level of preoperative bilirubin was the only significant risk factor for postoperative complications. Jaundice is associated with a higher risk of postoperative bleeding following PD and biliary drainage can increases the risk of septic complications.27 Although odds ratio of accompanying illness and intraoperative transfusion were also high, 2.67 and 3.04 respectively, these factors were not statistically significant, and no factors were associated with operative morbidity by multivariate analysis. These factors affect postoperative outcomes in other studies, but statistical insignificance in this study may be due to small case numbers. In this study, although the older patients had significantly more comorbid disease preoperatively, we could not find any significant differences in postoperative mortality and morbidity rates in the older group, and the age of the patient was not an independent risk factor for postoperative complications. Moreover, survival rates of older patients were comparable with younger patients. Richter et al. in 2002, had found that resections of cancers of the head of the pancreas are justified in patients over the age of 70 years, which is similar to our results.28 Their results showed that patients over 70 may have a more favorable long-term outcome than younger patients if the patient had ductal adenocarcinoma in the pancreatic head. They insisted that the resection is independent of age if there were no medical contraindications. These results and our data suggest that old age is not a reason for avoiding PD, and curative resection should be carried out in the elderly whenever oncologically feasible in the treatment of distal CBD cancer. Although in our study, combined disease was not an independent risk factor for postoperative morbidity, when patients had combined comorbid disease, the incidence of postoperative morbidity was higher, thus we should pay special attention to detecting and treating comorbid diseases before performing operations in the elderly.
In conclusion, surgical outcomes of elderly patients are similar to those of younger patients, despite a higher incidence of comorbid disease. These results provide evidence that PD can be applied safely to elderly patients.
Go to :
 XML Download
XML Download