

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Intraductal papillary mucinous neoplasm (IPMN) of the pancreas is a distinct entity characterized by papillary proliferations of mucin-producing epithelial cells with excessive mucus production and cystic dilatation of the pancreatic ducts. IPMN was first described by Ohashi et al. in 1982 and first recognized in the World Health Organization classification in 1996.1
IPMNs histologically show a broad spectrum ranging from adenoma to invasive carcinoma with different degrees of severity and seem to follow a progression from adenoma to invasive, similar to the well-defined adenoma-carcinoma sequence in colorectal cancer and pancreatic ductal adenocarcinoma (pancreatic intraepithelial neoplasia [PanIN] to invasive ductal carcinoma).23
Although prognosis for IPMN is better than that for ductal adenocarcinoma because IPMNs grow slowly and are diagnosed earlier than ductal adenocarcinoma, invasively transformed IPMNs have poor outcomes, similar to ductal adenocarcinoma. Thus, discriminating invasive IPMN from non-invasive IPMN is important for the choice of appropriate management of patients with IPMNs.
The purpose of this study was to determine predictive factors of invasive IPMN by examining and analyzing clinicopathological characteristics of the resected IPMNs.
Go to : 
METHODS
From February, 2001 to August, 2011, 36 patients with IPMNs underwent surgical resection in Kyungpook National University Hospital. Medical records and imaging findings of all patients were retrospectively examined for the presence of symptoms, tumor location, tumor size, maximum diameter of the main pancreatic duct (MPD), and presence of a mural nodule.
The diameter of main duct dilatation and the size of measurable mass lesions were used as independent continuous variables. According to the World Health Organization classification, the 36 resected IPMNs were pathologically described as non-invasive IPMN (IPMN with low-grade dysplasia, with intermediate-grade dysplasia, with high-grade dysplasia) and invasive IPMN (IPMN with an associated invasive carcinoma).
Statistical analysis of the data was performed using SPSS version 18.0. The difference in clinicopathological factors between non-invasive IPMNs and invasive IPMNs were analyzed by Student's t-test, chi-square test, or Fisher's exact test. A multivariate analysis was performed to determine the predictors of invasive IPMN using binary logistic regression. Receiver operating characteristic (ROC) curve analysis was used to analyze the sensitivity and specificity of possible cut-off values for the diameter of the main pancreatic duct and for mass size. ROC curves for the diameter of the main pancreatic duct were analyzed for 13 patients excluding pure branch-duct IPMNs. A similar ROC analysis was done for the size of the mass lesion among 26 patients excluding pure main duct IPMNs.
Go to :
RESULTS
Clinicopathologic characteristics of 36 patients with IPMNs
The mean age of the 36 patients with IPMN was 63.5±8.4 (range: 42-77) years. There were 21 males (58.3%) and 15 females (41.7%). Twenty one patients (58.3%) were symptomatic at presentation. A majority of patients (81%) presented with abdominal discomfort and pain. The mean size of the mass lesions was 32.5 mm (range: 10-70 mm) and the mean diameter of ducts was 4.9 mm (range: 1.0-14.2 mm). Most of the lesions were in the head of the pancreas (58.3%) (Table 1).
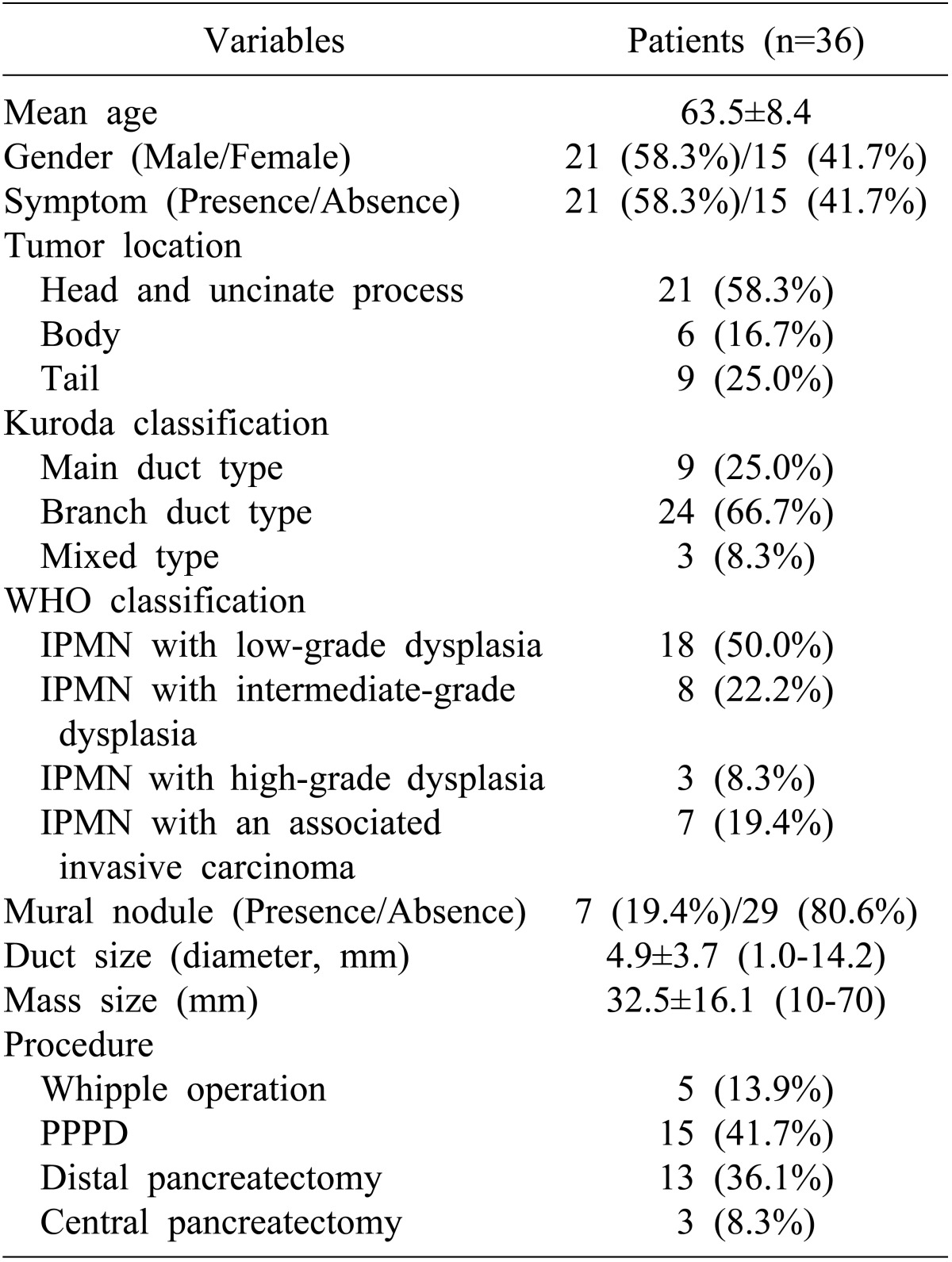
The histopathological diagnosis of the 36 resected IPMNs included 29 non-invasive IPMNs (IPMN with low-grade dysplasia [n=18], IPMN with intermediategrade dysplasia [n=8], and IPMN with high-grade dysplasia [n=3]) and 7 invasive IPMNs (IPMN with an associated invasive carcinoma) (Table 1).
Eight patients (22%) with IPMNs were associated with extrapancreatic neoplasms. Benign neoplasms were present in 5 cases (adrenal adenoma, 2; uterine myoma, 2; ampullary adenoma, 1); malignancies were present in 5 cases (gastric cancer [n=2], colon cancer [n=1], thyroid cancer [n=1], and cervical cancer [n=1]). Pancreatoduodenectomy was the most common operation and was performed in 20 cases (55.6%), 15 of which were pylorus-preserving operations. Distal pancreatectomy was performed in 13 cases (36.1%). Three patients (8.3%) underwent central pancreatectomy (Table 1).
Receiver operating characteristic curve analysis for cut-off values for the diameter of the main pancreatic duct and mass size
ROC curve analysis for cut-off values of the diameter of the main pancreatic duct and mass size was performed using data from the different patients group. ROC curve analysis for duct dilatation was done in 13 patients with duct dilatation excluding pure branch duct type IPMN. Using 7 mm as a cut-off level for the main duct diameter yielded a sensitivity of 100% and a specificity of 63%, whereas 8 mm yielded a sensitivity of 80% and a specifi city of 75% (Fig. 1A).
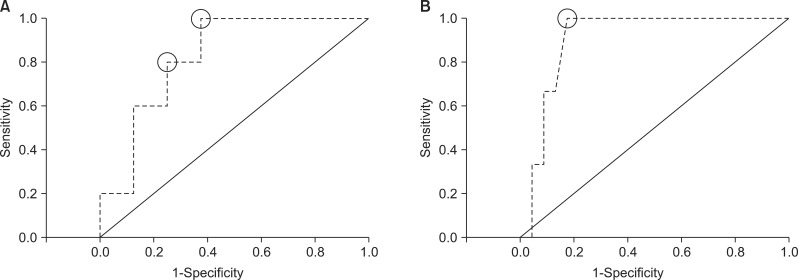 | Fig. 1Receiver operating characteristic curve analysis for cut-off values of the diameter of the main pancreatic duct and mass size. Using 7 mm as a cut-off level for the main duct diameter yielded a sensitivity of 100% and a specificity of 63%; 8 mm yielded a sensitivity of 80% and a specificity of 75% (A). Using 35 mm as a cut-off level for the size of the mass yielded a sensitivity of 100% and a specificity of 82.6% (B).
|
For the size of the mass lesion, ROC curve analysis was done in 26 patients with any measurable lesion dilatation excluding pure main duct type IPMN. Using 35 mm as a cut-off level for the size of the mass yielded a sensitivity of 100% and a specificity of 82.6% (Fig. 1B).
Univariate analysis between non-invasive IPMN and invasive IPMN
IPMN lesions were categorized as non-invasive IPMN and invasive IPMN by the WHO classification. There were 29 non-invasive IPMNs (80.6%) and 7 invasive IPMNs (19.4%). The mean age of the patients with non-invasive IPMN was 64.4±8.8 years, whereas the mean age of patients with invasive IPMN was 59.9±5.7 years. There were no significant differences between the 2 groups with regard to age, sex and symptoms. The mean size of the mass lesions of invasive IPMNs was larger than that of non-invasive IPMNs but the difference fell just short of significance (30.3±15.3 mm vs 47.0±15.0 mm; p=0.051). The mean diameter of the main pancreatic duct in invasive IPMN patients was significantly larger than that in non-invasive IPMN patients (4.1±3.2 mm vs 8.2±3 mm; p=0.007). A mural nodule was seen in preoperative imaging in 7 patients, Three (3 of 29 [10.3%]) patients had non-invasive IPMN and 4 (4 of 7 [57.1%]) invasive IPMN. The relationship between the presence of a mural nodule and invasive IPMN was significant (p=0.016) (Table 2).
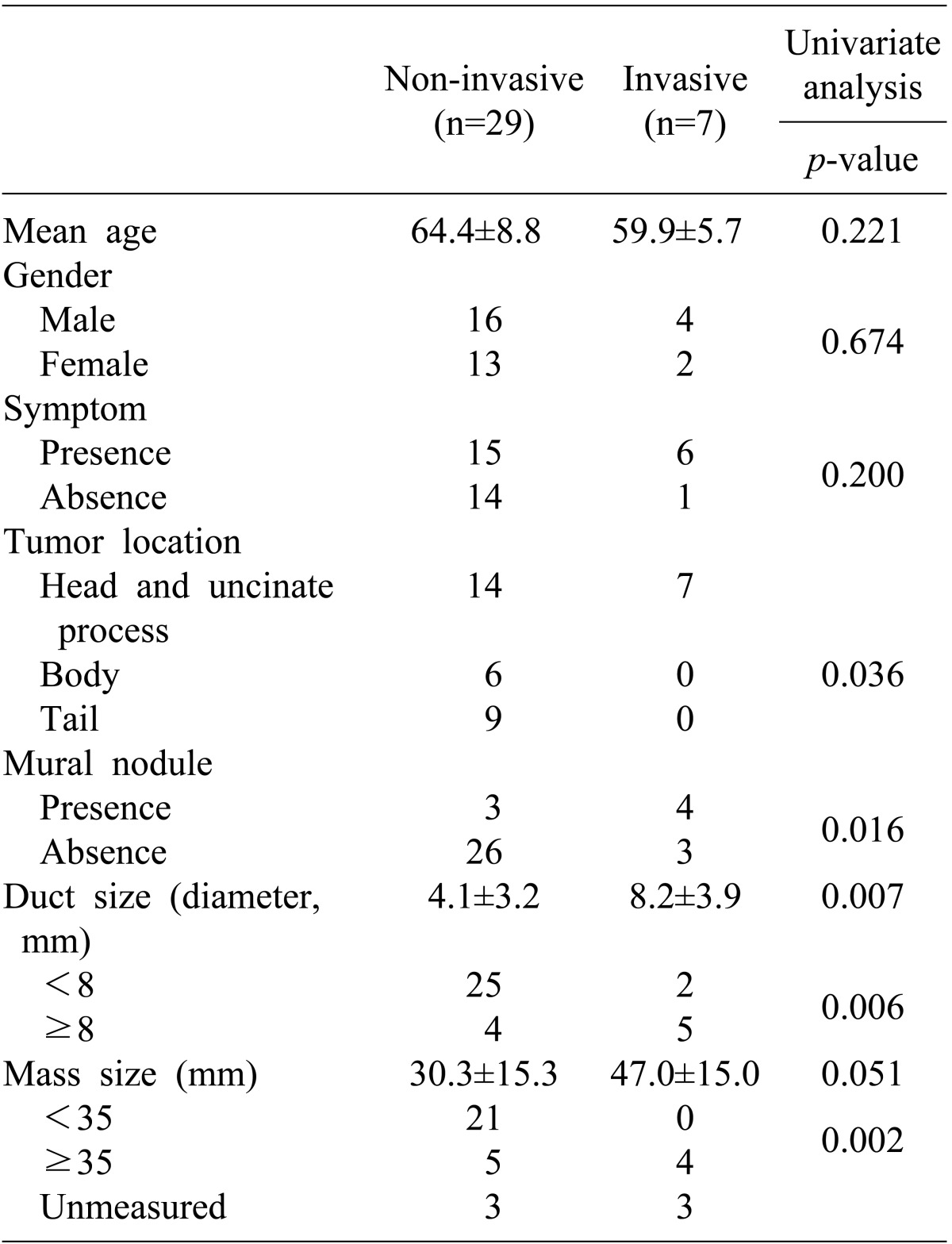
ROC curve analysis yielded optimal cut-off values for the diameter of the main pancreatic duct and mass size. Since an 8 mm diameter of the main pancreatic duct yielded high sensitivity (80%) and specificity (75%), we utilized 8 mm as the cutoff to divide patients into two groups. Nine patients had a main pancreatic duct diameter of 8 mm or greater including 4 patients out of 29 non-invasive IPMN patients (13.8%) and 5 patients out of 7 invasive IPMN patients (71.4%). A main pancreatic duct diameter of 8mm or greater was significantly more frequent in invasive IPMN (p=0.006). Similarly, since the 35 mm of mass size yielded high sensitivity (100%) and specificity (82.6%), we utilized 35 mm as a criterion to divide the patients into two groups. Nine patients had a mass size of 35mm or greater including 5 patients among the 26 non-invasive IPMN patients (19.2%) and 4 patients among 4 invasive IPMN patients (100%). A mass size of 35mm or greater was significantly more frequent in invasive IPMN (p=0.002) (Table 2).
Multivariate analysis between non-invasive IPMN and invasive IPMN
A multivariate analysis was performed to determine the independent predictors of invasive IPMN. The parameters of tumor size (<35 versus ≥35 mm), main duct dilatation (<8 versus ≥8 mm), symptoms (absent versus present), and mural nodules (absent versus present) were put into the binary logistic regression model. It showed that tumor size and mural nodule did not reach statistical significance. Among the factors verified by univariate analysis, main duct dilatation (≥8 mm) was the only significant factor predicting invasive IPMN (p=0.049) (Table 3).

Go to :
DISCUSSION
Recent advances in diagnostic imaging have resulted in an increased frequency of diagnosis for cystic mucin-producing pancreatic neoplasms. According to previous reports, IPMN represent about 1% of the pancreas exocrine tumors and about 12% of the pancreas cystic tumors.4 Two-thirds of IPMN patients are men. The peak age is the sixth decade. Despite the more frequent reporting of IPMN, the natural history of this disease is not well understood. How to manage patients with IMPNs, especially when it comes to timing of the surgical intervention, remains controversial.
Sonh et al.5 reported a lag-time of approximately 5 years from the time of development of an IPMN adenoma to the progression to IPMN with an associated invasive carcinoma. The incidence of invasive IPMN has been reported to be 0-35%.6
If an invasive component is present in IPMNs, the prognosis becomes unfavorable even after curative resection. The overall 5-year survival for patients with an invasive IPMN has been reported to range from 26 to 60%, compared with 90-95% in patients with a non-invasive component.7 Therefore, it is important to accurately differentiate malignant from benign IPMNs and select the appropriate treatment strategy.
The preoperative diagnosis and classification of IPMN is based upon imaging. In spite of advances in diagnostic imaging, it remains difficult to predict malignancy correctly4891011 and the accuracy is reported to be about 58-82%. The incidence of malignancy without malignant predicting factors in preoperative imaging was reported to be 10%.12 Thus, it is important to evaluate various clinical factors suggesting malignancy. Because prognosis of invasive IPMN is very poor, examination of predictive factors for invasive carcinoma is most important.
According to previous reports, tumor size, presence of a mural nodule, related symptoms, and dilatation of the main pancreatic duct have been reported to be important in predicting malignancy13141516171819; a mural nodule (≥6.3 mm) in the main pancreatic duct and a solid mass in pancreatic parenchyma were reported to be associated with invasive disease.11202122
In the present study, we tried to determine the sensitivity and specificity for invasive IMPNs of the diameter of the main pancreatic duct and the size of mass lesions using ROC curve analysis because these factors are continuous variables and have been reported as significant factors in previous reports. A cutoff of 8 mm for the main duct diameter and of 35 mm for the mass lesion size yielded both high sensitivity and specificity. We use these cutoff values as criteria to divide patients into groups for univariate and multivariate analysis.
Univariate analysis was performed to determine predictors of invasive IPMN. It showed that tumor location (p=0.036), mural nodule (p=0.016), and main duct dilatation (≥8 mm) (p=.006), and the size of mass lesion (≥35 mm) were statistically significant.
However, multivariate analysis showed that main ductal dilatation (≥8 mm) was the only independent predictive factor for invasive IPMN (p=0.049); tumor size and mural nodule fell just short of statistical significance. Failure of these two important factors, tumor size and mural nodule, to reach statistical significance may be related to the small number of cases in this study. Further studies enlarging the number of cases are required to determine the true significance in future studies.
In conclusion, IPMN is a premalignant lesion. It is important to distinguish invasive carcinoma from non-invasive IPMN. Our study showed that main duct dilatation ≥8 mm can be a useful indicator for predicting invasive IPMN.
Go to :
 XML Download
XML Download