

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cure of hepatic malignancy is deemed possible only if the tumor can be completely resected. However, it is difficult to resect an advanced hepatic malignancy that is huge and tightly invasive or adherent to adjacent organs, especially the inferior vena cava (IVC), hepatic vein, and diaphragm. The prognosis of the patient with primary liver cancer is dependent on the tumor stage, the degree of liver function impairment, and the underlying cirrhosis.1
Hepatocellular carcinomas (HCCs), as the majority of the hepatic malignancies, are considered unresectable if they are large, resulting in an insufficient hepatic remnant after resection; if they are extensive and/or multifocal in both lobes; if they are accompanied by extrahepatic metastases; or if they are associated with tumor thrombi in the main portal vein, hepatic vein, or IVC.2 The American Joint Committee on Cancer (AJCC) Staging 7th edition defines advanced HCC as above stage IIIA, if there are multiple tumors; if there is invasion of the portal or hepatic vein, or adjacent organs other than the gallbladder; or if the visceral peritoneum is perforated. For patients with this status, there is no standard treatment, and the role of surgery is still undetermined.3456
Recent reports have shown, however, that aggressive surgery may improve survival rates in patients with advanced HCC, even in the presence of poor prognostic factors, such as portal vein thrombosis or bilobar tumors.478 Similarly, salvage surgery following tumor down-staging with systemic chemotherapy and/or regional therapy has been reported to result in low operative mortality and morbidity and to provide better long-term outcomes,91011 we described here.
Seven patients who underwent difficult resections for advanced tumors with multiple metastases, invasion of adjacent organs, or pulmonary embolism, have experienced favorable outcomes. We also discuss the extension of indications for hepatectomy in patients with advanced hepatic malignancies.
Go to : 
METHODS
We describe 7 patients who underwent palliative or extensive surgery between July 2008 and March 2011 for advanced hepatic malignancies, including huge HCCs, intrahepatic cholangiocarcinoma (IHCC) with portal vein invasion, or repeated resection of metastatic carcinoma. Of the 7 patients, 3 were male and 4 were female; they ranged in age from 45-74 years. All had stage IV, except for one patient, who had a stage IIIC (T4N0M0) HCC according to AJCC 7th edition.
A review of patient records showed that patients had a history of the following: 1 had been diagnosed with hepatitis C virus (HCV)-associated HCC, 2 with hepatitis B virus (HBV)-associated HCC, 2 with IHCC with vascular invasion, and 2 had undergone repeated resections of recurrent IHCC or hepatic metastases of colon cancer. We recorded their demographic characteristics and medical history, such as chemotherapy or transarterial chemoembolization (TACE), the results of liver function tests (serum concentrations of aspartate transaminase [AST], alanine transaminase [ALT], bilirubin, alkaline phosphatase, albumin, and prothrombin time), assays of tumor markers (alpha-fetoprotein [AFP], protein-induced by Vitamin K absence or antagonist-II (PIVKA-II], carcinoembryonic antigen [CEA], and carbohydrate antigen 19-9 [CA19-9]), results of indocyanine green retention test at 15 minutes (ICG R15), imaging modalities, such as contrast-enhanced computed tomography (CT) or magnetic resonance imaging (MRI), and intraoperative and pathologic findings. These results are summarized in Table 1.
Table 1
Summary of the characteristic of the patients
OS, overall survival; DFS, disease-free survival; IHCC, intrahepatic cholangiocarcinoma; HCC, hepatocellular carcinoma; RH, right hemihepatectomy; LND, lymph node dissection; pRTS, palliative right trisectionectomy; HV, hepatic vein; RTS, right trisectionectomy; TVE, total vascular exclusion; IVC, inferior vena cava; PTE, pulmonary thromboembolism; LH, left hemihepatectomy; AR, anterior resection; PH, partial hepatectomy; RTx, radiotherapy; TACI, transarterial chemoinfusion; CTx, chemotherapy; Op, operation.
![]()
Go to :
RESULTS
Patient 1
Patient 1 was a 53-year-old woman with a 6 cm-sized mass in segment VIII. She had undergone an open cholecystectomy 24 years earlier. Her preoperative liver function and tumor marker tests gave normal results. She was diagnosed with an IHCC with left portal vein invasion and of clinical stage IVA (T2N1M0). We performed a right hemihepatectomy including S4b, resection of the bile duct, left portal vein, and lymph node dissection. On gross examination, this patient was found to have a mass-forming type of IHCC, and on microscopic examination, she was diagnosed with an adenocarcinoma with moderate differentiation, vascular invasion, and perineural invasion, with tumor cell spread to the 12p lymph node; the final staging was IVA (T3N1M0). The surgery was uneventful, and she underwent radiotherapy for one month postoperatively. At 39 months after surgery, the patient was surviving with no evidence of tumor recurrence or metastasis.
Patient 2
Patient 2 was a 74-year-old man with chronic hepatitis C infection, hypertension and a history of tuberculosis pleurisy about 55 years earlier. Preoperatively, his PIVKA-II level was elevated highly (>2,400 mAU/ml) and his serum HCV RNA was 2.3×105 IU/ml. Imaging showed multiple, variable sized masses in the right hepatic lobe and segment IV, variable sized nodules in both lungs and an about 1 cm-sized nodule in the left adrenal gland. The largest liver mass was more than 10 cm in size. His preoperative liver function test was in normal range except ICG R15 of 15.6%. We performed a palliative right trisectionectomy. Pathologic examination showed an HCC of trabecular and hepatic types, scored as Edmondson-Steiner Grade 3/2. Microscopically, the tumor showed vascular invasion and multiple satellite nodules. After the surgery, he underwent transarterial chemoinfusion (TACI) twice, followed by regular treatment with sorafenib. At present, 38 months after surgery, the patient remains alive with the improvement of quality of life in spite of residual pulmonary metastases.
Patient 3
Patient 3 was a 50-year-old man with HBV-associated HCC before surgery. He had a huge mass replacing his right hemiliver with malignant thrombosis in the right posterior portal vein and invasion of the right and middle hepatic veins (Fig. 1A, B). His serum AFP concentration was 298,000 ng/ml. He had started to take sorafenib at the time of diagnosis and underwent TACE before surgery. His preoperative levels of AST and ALT were mild elevated (89/57 IU/L) and prothrombin time was mildly prolonged (74.4%). We performed a right hemihepatectomy, diaphragm excision due to invasion, evacuation of tumor thrombus from the hepatic vein, venoplasty of the right hepatic vein and inferior vena cava (IVC) with total vascular exclusion. The tumor was an 11.5×10×6.8 cm-sized HCC with invasion of the diaphragm and portal vein thrombosis (Fig. 1C). Despite bad results on a preoperative ICG R15 of 26.7%, he had good postoperative course, and underwent TACI after the surgery. For 12 months after surgery, imaging revealed no unusual postoperative findings and was maintained on sorafenib (Fig. 1D).
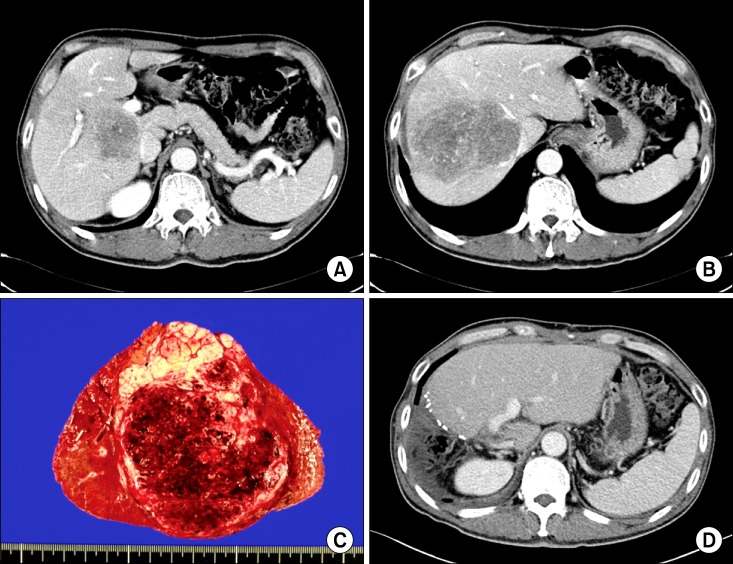 | Fig. 1Images of patient 3. (A, B) Initial liver dynamic CT scan showing a huge hepatocellular carcinoma with thrombi in the right hepatic vein and portal vein and intrahepatic metastases. (C) Photograph of the gross specimen, showing a multinodular confluent, trabecular, and hepatic type of hepatocellular carcinoma, of Edmondson-Steiner grade 4/3, measuring 11.5×10×6.8 cm with invasion of diaphragm, and portal vein thrombus. (D) CT scan of 12 months after surgery showing no evidence of recurrence or metastasis in the retained left hepatic lobe.
|
Patient 4
Patient 4 was a 67-year-old man with HBV-associated HCC. His AST/ALT was mildly elevated preoperatively (140/87 IU/L), and his PIVKA-II level was very high (> 20,000 mAU/ml). Imaging showed two large (10 and 11 cm) nodular HCCs and three tiny intra-hepatic metastatic lesions in the left lobe, tumor thrombus in the right hepatic vein and thromboembolisms in both pulmonary arteries. He was staged clinically stage IVB. Before the operation, he received an IVC filter to prevent aggravation of the pulmonary thromboembolism, and after the operation he started anticoagulation therapy. We performed a right trisectionectomy with partial resection of the diaphragm and partial hepatectomy for a small lesion on the left hemiliver, and total vascular exclusion. Pathology showed 2 large tumors measuring 15 and 10.8 cm on the right hemiliver and one small (0.7 cm) HCC on segment 3. After the operation, the patient recovered well without complications. The patient has continued chemotherapy with sorafenib, along with anticoagulation therapy. At 6 months after surgery, he shows no evidence of recurrent HCC.
Patient 5
Patient 5 was a 45-year-old previous healthy woman with a 5 cm-sized IHCC in the caudate lobe and invasion of the IVC and main portal vein (Fig. 2A, B). At the time of diagnosis, her CA19-9 level was 88.6 U/ml. After 1 month of preoperative chemo- and radio-therapy, she underwent a left trisectionectomy and resection of the IVC. During the operation, we resected the IVC which had been invaded by the tumor, followed by an anastomosis by interpositioning the graft with total vascular exclusion (Fig. 2C-G). Pathologic examination showed that the tumor was a mass forming type of cholangiocarcinoma, measuring 5.8×5.0×4.2 cm with poor differentiation and invading the IVC (Fig. 2H). Twenty months after surgery, this patient showed no evidence of recurrence or metastases despite an IVC thrombus with venous congestion. The patient is currently receiving anticoagulation therapy and was waiting for a thrombectomy.
 | Fig. 2Images of patients 5. (A, B) Initial CT scan showing an intrahepatic cholangiocarcinoma on the caudate lobe with intrahepatic inferior vena cava invasion and abutting the main portal vein. (C-G) Intraoperative photographs during left hemihepatectomy, caudate lobectomy, inferior vena cava resection and interposition graft and total vascular exclusion through individual approach. (H) Photograph of a gross specimen, showing that the tumor was a mass forming type of cholangiocarcinoma with poor differentiation, measuring 5.8×5.0×4.2 cm and invading the inferior vena cava.
|
Patient 6
Patient 6 was 64-year-old woman who underwent a right posterior sectionectomy in June 2003 for a mucinous type of IHCC measuring 5×2.5×2.4 cm in size. Six years later, this patient was found to have a recurrent IHCC on the right anterior section, for which she underwent a right hemihepatectomy, S1, and bile duct resection. At that time, the recurrent tumor was diagnosed pathologically as a mucinous, intraductal growth type of cholangiocarcinoma with moderate differentiation, measuring 4.5×3.2× 2.1 cm in size and accompanied by lymph node metastases. One year later, we observed enlargement of a para-aortic lymph node, which was dissected surgically, followed by adjuvant chemotherapy. At 20 months after last surgery, the patient remained alive despite the increase of size and number of recurrent tumors.
Patient 7
Patient 7 was a 49-year-old man who had previously undergone surgery for colon cancer with liver metastasis, consisting of palliative right hemihepatectomy and caudate lobectomy, diaphragm resection, and anterior resection of the colon. However, the metastatic mass in the liver recurred twice at 1-year intervals, for which the patient underwent repeated resections, followed by 34 doses of chemotherapy. At 17 months after last surgery, he remained free from cancer.
Go to :
DISCUSSION
Identification of the optimal therapeutic approach to patients with advanced hepatic malignancy represents a difficult challenge.5 Several modalities, however, are available to treat advanced hepatic malignancies. Locoregional treatments include surgery, radiofrequency ablation, transarterial chemoembolization, and percutaneous ethanol injection, whereas systemic treatments include chemotherapy and sorafenib. The criteria for palliative treatments are less well-defined in patients with advanced hepatic malignancies, due to the poor efficacy of each form of therapy.12 Nevertheless, palliative therapy may induce good responses and even improve long-term survival in some patients.13 Since these modalities may be single or combined, a multi-disciplinary approach is needed to treat patients with advanced hepatic malignancy. Among the options available for surgeons are total vascular exclusion, repeated surgical resection, lymph node dissection, vascular repair and metastasectomy.
Another approach consists of the down-staging of unresectable tumors, due to the local extent of disease or distant metastases. Relatively little is known, however, about the outcomes of tumor downstaging followed by salvage liver resection, and it is unclear whether this strategy provides long-term survival comparable to primary resection of resectable tumors. Salvage surgery after tumor downstaging has been shown to yield good long-term results and the possibility of cure in some patients with unresectable tumors.291011
Although all 7 of these patients described here had advanced hepatic malignancies with intra- or extrahepatic metastases, invasion of adjacent structures or repeated recurrence after resection, all had excellent general performance status with good liver function. In general, the main cause of death in patients with advanced hepatic malignancy is liver failure caused by the increased tumor mass or venous thrombosis in the liver prior to multiple extrahepatic metastases or the failure of other organs, such as the kidneys or lungs.12 Prior to performing surgery on these carefully selected patients, we believed that they would tolerate major hepatectomy with a low rate of possible morbidities, that we could resect the entire intrahepatic mass aggressively and attempt adjuvant treatment with systemic chemotherapy or sorafenib. Therefore, we performed extensive and palliative surgery on 7 patients with advanced hepatic malignancy, and observed their favorable outcomes.
IHCC accounts for approximately 5% to 10% of all primary hepatic malignancy.14 Although extended hepatectomy, extrahepatic bile duct resection, and lymph node dissection have been performed in these patients, those with the mass-forming type of IHCC had better surgical outcomes, including rates of survival and local recurrence, than patients with the mass-forming plus periductal infiltrating type of IHCC.15 Extended hepatectomy with complete tumor removal has been reported to be the only treatment strategy that can prolong survival in patients with IHCC.16 Although the role of regional lymphadenectomy remains unclear, the presence of lymph node metastases may be an unfavorable prognostic factor in patients with IHCC.17 Our findings, however, suggest that aggressive hepatectomy and lymph node dissection can enhance long term survival. We therefore performed extended hepatectomy with complete tumor removal and lymph node dissection, despite the difficulty in complete resection of these tumors. Based on these positive outcomes, radiotherapy or systemic chemotherapy, in addition to surgery, should be considered in patients with IHCC.15
Likewise, hepatic resection for metastatic colorectal cancer has been found to be optimal for long-term survival and cure.18 Many effective chemotherapy regimens have been described for patients with colorectal cancer, and these regimens have improved the resectability and survival of patients with advanced hepatic metastases.19 In addition, advances in surgical strategy for hepatectomy, such as portal vein embolization, 2-stage hepatectomy, multiple partial hepatectomy, and/or radiofrequency ablation under intraoperative ultrasonography guidance, and repeated hepatectomy, have allowed patients with greater burdens of metastatic disease to undergo complete operative resection.18192021 Overall, these factors have led to an expansion of indications for hepatectomy for colorectal cancer metastases.19
This study had several limitations, including retrospective design and a small number of patients. Thus, it is difficult to determine an overall strategy to treat heterogeneous types of advanced hepatic malignancies. Moreover, it would be difficult to perform a randomized controlled trial of these patients. Another limitation was the heterogeneity of this group of patients. However, selecting groups of patients with the same stage or disease entity may yield more consistent results.
In highly selected patients with stage 3 or 4 hepatic malignancies, aggressive surgical approaches may prolong survival, while maintaining a good quality of life, despite residual macroscopic intra- or extrahepatic metastases. Surgery remains the key therapeutic modality to treat the patients with advanced hepatic malignancies.
Go to :
 XML Download
XML Download