

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
A rapid and accurate reduction is important for hip dislocated patients to avoid various potential complications, including avascular necrosis of the femoral head. We analyzed hip dislocation cases, ones that particularly failed during the primary reduction trial.
Materials and Methods
Eighty-seven patients with hip dislocation, who visited the emergency department between January 2007 and September 2015, were retrospectively analyzed. Of them, 68 patients were successfully treated in the first closed reduction trial, and the remaining 19 patients were unsuccessful. Of the 19 unsuccessful first trial, 12 patients were successfully treated in the second closed reduction; however, in the remaining 7 patients, open reduction was performed in the operation room with general anesthesia. Every closed reduction was practiced by at least 2 orthopedic doctors, and open reduction was performed by a single senior author.
Results
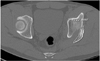
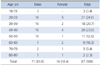
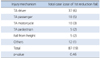
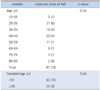
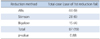
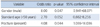
The rate of first reduction failure was higher, with statistical significance, in patients aged under 50 years, male gender, and those with combined around hip fractures, including femoral head and acetabular fracture (p<0.05). In particular, the presence of impacted fracture fragment in the hip joint and large size of the impacted fracture fragment was highly related to the failure of second closed reduction trial requiring open reduction. Conversely, the method of reduction, Thompson-Epstein classification, Pipkin classification were not related to the failure of closed reduction statistically (p>0.05).
Conclusion
To evaluate the patients with hip dislocation, realizing the type of dislocation, presence of accompanied fracture, location and size of fracture fragment, age, as well as gender of patients is important. If the fracture fragment is impacted in the hip joint and the size of the fragment is large, then the operative treatment is considered, rather than the repetitive trial of closed reduction by constraint.



References
1. Campbell WC, Canale ST, Beaty JH. Campbell's operative orthopaedics. 12th ed. Philadelphia: Mosby;2013.
2. Moed BR, Reilly MC. Acetabulum fractures. In : Bucholz RW, Court Brown CM, Heckman JD, editors. Rockwood and Green's fractures in adults. 7th ed. Philadelphia (PA): Lippincott Williams & Wilkins;2010. p. 1463–1523.
3. Rosenthal RE, Coker WL. Posterior fracture-dislocation of the hip: an epidemiologic review. J Trauma. 1979; 19:572–581.
4. Sah AP, Marsh E. Traumatic simultaneous asymmetric hip dislocations and motor vehicle accidents. Orthopedics. 2008; 31:613.

5. Sanders S, Tejwani N, Egol KA. Traumatic hip dislocation--a review. Bull NYU Hosp Jt Dis. 2010; 68:91–96.
6. Hougaard K, Thomsen PB. Traumatic posterior dislocation of the hip: prognostic factors influencing the incidence of avascular necrosis of the femoral head. Arch Orthop Trauma Surg. 1986; 106:32–35.
7. Paus B. Traumatic dislocations of the; late results in 76 cases. Acta Orthop Scand. 1951; 21:99–112.
8. Stewart MJ, Milford LW. Fracture-dislocation of the; an endresult study. J Bone Joint Surg Am. 1954; 36:315–342.
9. Brav EA. Traumatic dislocation of the hip: Army experience and results over a twelve-year period. J Bone Joint Surg Am. 1962; 44:1115–1134.
10. Tornetta P 3rd, Mostafavi HR. Hip dislocation: current treatment regimens. J Am Acad Orthop Surg. 1997; 5:27–36.
11. Thompson VP, Epstein HC. Traumatic dislocation of the; a survey of two hundred and four cases covering a period of twenty-one years. J Bone Joint Surg Am. 1951; 33:746–778.
12. Proctor H. Dislocations of the hip joint (excluding 'central' dislocations) and their complications. Injury. 1973; 5:1–12.
13. Hunter GA. Posterior dislocation and fracture-dislocation of the hip. A review of fifty-seven patients. J Bone Joint Surg Br. 1969; 51:38–44.
14. Paterson I. The torn acetabular labrum; a block to reduction of a dislocated hip. J Bone Joint Surg Br. 1957; 39:306–309.
15. Thompson SM. Traumatic dislocation of the hip. In proceedings of the Sheffield regional orthopaedic club. J Bone and Joint Surg. 1960; 42:858.
16. Epstein HC, Harvey JP. Traumatic anterior dislocation of the hip. Management and results. J Bone Joint Surg Am. 1972; 54:1561–1570.
17. Pipkin G. Treatment of grade IV fracture-dislocation of the hip. J Bone Joint Surg Am. 1957; 39:1027–1042.
18. Keith JE Jr, Brashear HR Jr, Guilford WB. Stability of posterior fracture-dislocations of the hip. Quantitative assessment using computed tomography. J Bone Joint Surg Am. 1988; 70:711–714.
19. Magu NK, Magu S, Rohilla RK, Batra A, Jaipuria A, Singh A. Computed tomographic evaluation of the proximal femur: a predictive classification in displaced femoral neck fracture management. Indian J Orthop. 2014; 48:476–483.
20. Canale ST, Manugian AH. Irreducible traumatic dislocations of the hip. J Bone Joint Surg Am. 1979; 61:7–14.
21. Mullis BH, Dahners LE. Hip arthroscopy to remove loose bodies after traumatic dislocation. J Orthop Trauma. 2006; 20:22–26.
22. Lima LC, do Nascimento RA, de Almeida VM, Façanha Filho FA. Epidemiology of traumatic hip dislocation in patients treated in Ceará, Brazil. Acta Ortop Bras. 2014; 22:151–154.
23. Alonso JE, Volgas DA, Giordano V, Stannard JP. A review of the treatment of hip dislocations associated with acetabular fractures. Clin Orthop Relat Res. 2000; (377):32–43.
24. Sahin V, Karakaş ES, Aksu S, Atlihan D, Turk CY, Halici M. Traumatic dislocation and fracture-dislocation of the hip: a long-term follow-up study. J Trauma. 2003; 54:520–529.
25. Brock G. The occasional posterior hip dislocation reduction. Can J Rural Med. 2015; 20:65–70.
26. Dwyer AJ, John B, Singh SA, Mam MK. Complications after posterior dislocation of the hip. Int Orthop. 2006; 30:224–227.
27. Terjesen T, Horn J, Gunderson RB. Fifty-year follow-up of late-detected hip dislocation: clinical and radiographic outcomes for seventy-one patients treated with traction to obtain gradual closed reduction. J Bone Joint Surg Am. 2014; 96:e28.
28. Pan J, Bredella MA. Imaging of soft tissue abnormalities about the hip. Radiol Clin North Am. 2013; 51:353–369.
 XML Download
XML Download