

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Acromioclavicular (AC) joint dislocation is common injury of shoulder related to sports medicine and orthopedics.12) Recently AC joint injury has been a significantly increasing due to increasing rate of traffic accident, sportrelated leisure activity and industrial accident. The Rockwood classification is used most commonly for AC joint dislocation.2) It is classified as 6 stages by the damage of AC ligament and coracoclavicular (CC) ligament.3) Surgical treatment is commonly applied in cases of more than type IV injury of Rockwood classification. There is some controversy for treatment plan of type III injury, but surgical treatment is accepted for young patients, athletics, physical labor, cases of cosmetic dissatisfaction of dislocated AC joint.34567)
The surgical treatment is focused on recovery of the distance between coracoid and clavicle, and maintenance of stability.28) B ecause of t he d ifficulty i n reconstructing anatomic structure of CC ligament, surgical treatment uses the augmentation of structures for stability. There are several methods: (1) the fixation between coracoid process and clavicle, (2) the fixation of AC joint, (3) the fixations with AC joint and CC joint both, (4) the resection of distal clavicle, (5) the transfer of muscles.2891011) However, the clinical superiority of these procedures remains debatable, and various complications have been reported.
Recently, the open reduction and fixation by Hook plate (DePuy Synthes, Zuchwil, Switzerland) and CC ligament augmentation by TightRope (Arthrex, Naples, FL, USA) are commonly used methods due to their good reported clinical outcomes.1112131415) The Hook plate fixation is the method that fixes between distal clavicle and acromion by plate. It can easily maintain the reduction without direct injury of AC joint surface, and it has relatively simple technique with minimal incision and can make the early range of motion (ROM) of joint.14) TightRope fixation is the method that ties up the CC joint by non-absorbable band. It has advantages of maintaining the reduction with minimal incision without AC joint surface injury like the hook plate fixation, and it doesn't need to hardware removal.13)
Although these two methods have advantages of being relatively lesser invasive with better outcome compared to other methods, there is only a few clinical studies about comparison between the two.12161718) The purpose of this study was to retrospectively evaluate the clinical and radiological outcomes of Hook plate fixation and CC ligament augmentation using TightRope in acute AC joint dislocation.
MATERIALS AND METHODS
Total 51 consecutive (32 Hook plate fixation, 19 TightRope fixation) patients with acute AC joint dislocations were reviewed for this study from May 2009 to May 2012.
We selected the patients with the following criteria: (1) adults with acute, closed, and higher lesion than Rockwood type III of AC joint dislocation or; (2) fixation with clavicular hook plate or TightRope; (3) normal shoulder function before injury; (4) without associated injuries; (5) regular follow-up more than 12 months postoperatively. Whereas those with (1) fracture at clavicle or acromion, (2) history of surgical intervention to the shoulder girdle, (3) ipsilateral accompanied damage in same upper extremity, or (4) history of shoulder stiffness were excluded.
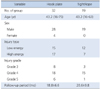
The patients were divided into two groups according to the surgical methods. Thirty-two patients were stabilized with Hook plate fixation (HP group). Nineteen patients were treated with TightRope (TR group). The demographics and injury mechanisms related to the two groups are shown in Table 1.
1. Operative technique and postoperative care
1) Open reduction and fixation with Hook plate
Under general anesthesia, the patient was placed in the supine position. A skin incision was made from end of acromion to medial side of coracoid process (Fig. 1A). After subcutaneous dissection, AC joint and CC ligament were exposed. The space was made for Hook plate (locking complession plate [LCP] clavicle hook plate; DePuy Synthes) insertion site at soft tissue of AC joint posterior side. The hook plate was inserted into the space to reach the lower part of acromion. The reduction was done using the down side pressure on clavicle part of plate. At that time, acromion was used like a lever. Before insertion of screw, authors confirmed the position of acromion and clavicle, over reduction and contact position of hook at acromion using radiographic image amplifier (Fig. 1B). Screw was inserted to maintain the reduction. The skin sutures and aseptic dressing were performed. Abduction brace was applied for 1 to 3 weeks depending on the patient's pain. Gentle pendulum exercise was encouraged postoperatively under the protection. However active forward flexion and abduction over 90° was not encouraged until Hook plate removal to reduce potential irritation of the acromion or impingement of the rotator cuff. According to the manufacturer's guidelines, the Hook plate were removed usually approximately 3 months after fixation, After implant removal, a free motion was allowed. The sport activities were not allowed for 3 months.
2) CC ligament augmentation using TightRope
Under general anesthesia, the patient was placed in the supine position. A skin incision was made the medial side of AC joint. After dissection of subcutaneous tissue was done, the authors made a hole at CC ligament attach site of distal clavicle (mid-portion between conoid and trapezoid ligament). The lower part of coracoids process was exposed and neuro-vascular structure were protected by Homan retractor, then the authors made a hole there. A shuttle wire (cerclage wire, 0.6 mm; DePuy Synthes) was passed through from the hole of clavicle to the hole of coracoid process, and made a connection with TightRope (Arthrex) which is passed through the two holes. After manual reduction of AC joint, the author maintained reduction until fixing the TighRope by the K-wire through lateral side of acromion to distal clavicle (Fig. 1C).
We remained the K-wire fixation to correct anteroposterior translation of distal clavicle to acromion when anteroposterior instability was remaining during surgical procedure.
After fixing the TightRope, skin sutures and aseptic dressing was done. Abduction brace was applied for 1 to 3 weeks depending on patient's pain. Gentle pendulum exercise was encouraged postoperatively under the protection. However active forward flexion and abduction over 90° were limited to prevent K-wire breakage until K-wire removal after 6 weeks of surgery. From the 7th week, a free motion was allowed. The sport activities were not allowed for 3 months.
2. Clinical evaluation and statistical analysis
All of our patients could be reviewed and examined during the follow-up study. All participants were received monthly radiographs and clinical follow-up after operation. The follow-up evaluations were performed in a standardized fashion by two independent examiners.
Final clinical and radiological assessments were performed at a mean of 19.5±7.9 months after operation. The mean follow-up period was 18.8±6.6 months in the HP group and 20.6±9.8 months in the TR group (p=0.430).
For radiographic evaluation, shoulder X-ray was taken in all patients before and after the internal fixation surgery, before and after the removal of the implant (Hook plate in HP group, K-wires in TR group) and final visit. To evaluate the results of reduction of the AC joint after surgery, the coracoclavicular distance (CD, height between the upper border of the coracoid process and the inferior cortex of the clavicle) was measured in each side and the increase of height on the operated side was compared to the unaffected side and calculated in percent (comparative coracoclavicular distance, CCD). Moreover, the radiographs were evaluated for acromial osteolysis and presence of posttraumatic osteoarthritis which may or not accompanied by clinical symptom.
Clinical outcomes were assessed using Constant score, University of California at Los Angeles (UCLA) score, Korea shoulder score (KSS) and recovery of ROM in a standardized fashion by two independent examiners. Furthermore, we performed cross-body adduction test to check clinical relevance to radiologic AC joint osteoarthritis in all patients.19)
Descriptive statistical analyses were performed using SPSS ver. 15.0 (SPSS Inc., Chicago, IL, USA). Kolmogorov-Smirnov test were determined normality of the tested variables and chi-square test was applied for classification variables; t-test was used for continuous variable. A p-value less than 0.05 were considered statistically significant.
Results
In group HP, 32 patients were 28 male, 4 female; mean age 43.2 years (range, 16-75 years). The group included 15 patients of low energy injury like fall form height or contact sports, 17 patients of high energy injury like vehicle accident. Injuries were documented by preoperative plain X-rays of the affected shoulder in the anteroposterior (AP) standing, axillary views, and AP in stress mode. The numbers of injury were 8 type III dislocations, 18 type IV dislocations, 6 type V dislocations. Mean follow-up period was 18.8±6.6 months.
In group TR, 19 patients with TightRope fixation were 19 male, no female with mean age 43.2 years (range, 16-63 years). They included 12 patients of low energy injury, 7 patients of high energy injury. The number of each injury types was 3 type III dislocations, 15 type IV dislocations, 1 type V dislocations. Mean follow-up period was 20.6±9.8 months (Table 1).
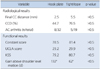
With regard to the clinical outcomes, at the final follow-up, HP group were rated 78.5 (range, 46-93) of constant score, 29.2 of UCLA score (range, 11-34), 79.2 of KSS (range, 46-95). TR group were rated 81.4 of constant score, 29.9 of UCLA score, 80.7 of KSS, respectively (Table 2). These clinical scores (Constant score, UCLA score, KSS) presented good results in both groups without a significant difference.
Furthermore we examined the ROM recovery after each operation; patients who were operated with Hook plate appeared to gain ROM of shoulder relatively slower. It takes 132 days to gain above shoulder level motion in HP group and 62 days in TR group, respectively. These showed a significant difference (p<0.05). But, in two weeks after removing the plate, the shoulder function was significantly improved, the ROM at final visit revealed almost the same results in both groups. Mean ROM at final visit in forward flexion and abduction revealed 174.1° (150°-180°)/170.6° (150°-180°) in the HP group and 176.5° (150°-180°)/172.6° (160°-180°) in the TR group (p=0.37/p=0.45).
With regard to the radiologic outcomes, at the final follow-up, both group revealed little difference in vertical distance in shoulder AP view (Fig. 2). The patients with Hook plate showed mean 2.5 mm vertical distance in shoulder AP view, while the patients with TightRope was mean 5.5 mm vertical distance in shoulder AP view (p=0.29). The CCD (which were compared to the unaffected side and calculated in percent) increased to 44.7% (0%-300%) in the HP group and to 76.5% (0%-250%) in the TR group at final follow-up, but no one was significantly superior to others (p=0.19).
All of case had no early reduction failure and re-dislocation. In 14 patients (43.8%) with HP fixation, subacromial osteolysis around hook had been seen in follow-up radiograph, but serious Hook plate related complications such as hook perforation through acromion, acromial fracture or fixation failure were not observed. And subacromial osteolysis did not represent clinical inferiority in patients. In five patients in TR group, button sinking had been seen due to bony absorption under clavicular side cortical button but patients had no symptom.
The posttraumatic radiographic change (e.g., AC joint space narrowing, bony sclerosis or osteophyte after AC joint dislocation) was seen 8 cases of 32 AO hook plate, 5 cases of 19 TightRope in their follow–up (Fig. 3). And most patients with radiographic arthritic change had no arthritic symptom such as resting pain or aggravation of pain on cross-body adduction test. A poor correlation between clinical and radiological results with regard to the AC joint arthritis was observed (p=0.39).
Deep infection and nerve injury did not exist in both group, but subcutaneous infection appeared to one case in each group. The both of them were resolved with oral antibiotics and healed uneventfully without further surgery.
Discussion
In the current study, we compared the results between two surgical methods including clavicular Hook plate and CC fixation with TightRope. The most important finding of the present study was that the outcome of the clavicular Hook plate fixation was at least equal to the results, which could be achieved CC fixation with TightRope for the treatment of acute AC joint separations.
According to clinical shoulder rating scale and scores (Constant score, UCLA score, KSS), we found that both surgical methods can have similar and good functional results at final visit (at least 1 years follow up after the surgery) and almost present normal shoulder function.
Hook plates provide a non-rigid fixation allowing normal rotation between the clavicle and the scapula, as well as secure fixation for AC joint reduction. The hook plates establish a non-rigid fixation to maintain normal biomechanical rotation and subsequently allow a longer period for retention of the implant, ensuring adequate healing of the fracture and coraco-clavicular ligaments.1420)
Although the clavicular hook plate provided excellent results, this implant may cause rotator cuff injury, subacromial impingement, and acromial fracture.1721) ElMaraghy et al.22) reported that the subacromial hook resulted in subacromail bursal penetration and the subacromial space is limited. Because of bursal inflammation and rotator cuff impingement, the HP group had the worse ROM which may have resulted from the pain during shoulder movement. There were varying degrees of shoulder dysfunction due to the Hook plate, and the shoulder function was significantly improved after removal of the plate, indicating a close correlation of hook plate implant with shoulder dysfunction.21) Furthermore Fung's cadaveric mechanical studies suggest that if arm elevation is less than 90°, the relative rotation of the clavicle against the shoulder is small; but if arm elevation is more than 90°, the rotation of the clavicle becomes significant. Especially when the hook of the plate is positioned under subacromial surface and in close contact it, the rotation of the clavicle is limited, which may cause difficulties in the elevation of the shoulder after surgery.23)
During follow-up, we found that patients the shoulder pain was not severe, when shoulder motion was poor, especially it was hard for the upper limbs to be raised more than 90°.
In our rehabilitation program, active forward flexion over 90° and abduction above shoulder were not encouraged until implant removal after 12 to 16 weeks of surgery to decrease potential irritation of the acromion or impingement of the rotator cuff in the HP group. Our conservative rehabilitations may cause late recovery of ROM above shoulder level in the HP group (mean, 132 days) compared to the TR group (mean, 62 days).
All the patients in the HP group received implant removal at the mean time of 121±34 days and then authors accelerated maximum ROM exercise after remove. In two weeks after removing the plate, the shoulder function was significantly improved; eventually we could find that the ROM did not differ significantly between the two groups at 12months and final visit. Chen et al.21) also found that the shoulder function was significantly improved after the hook plate was removed.
The TightRope was developed for reduction of vertical instability and maintenance of coraco-clavicular distance as the fixation procedure between coracoid process and clavicle.1324) Due to the advantage of stable fixation power and needlessness of removal procedure, it was introduced for arthroscopic and open reduction and fixation of AC joint dislocation, and became popular.132526) Especially, some authors advocated that Arthroscopic stabilization of acute ACJ dislocations using a single TightRope implant is an elegant minimally invasive method with good results in indicated cases, but they also reported loss of full reduction on radiographs more frequently, although no effect on the clinical outcome is evident.27) In this study, we operated patient with open technique, because arthroscopic method has some limitations such that it requires higher skill of the surgeon, costs higher, so only few surgeons can apply for acute AC dislocation injury.
And, most cases in the TR group (18/19); the additional use of K-wire with tight rope was done to provide better AP reduction of AC dislocation. We left these two trans acromion-clavicle K-wires for 6 weeks to reach a better fixation and to allow a better healing and scaring of residual ligaments. Until remove of K-wires, there were no K-wire related complications such as metal breakage or neurovascular damage by migration. Sometimes an osteolysis (2 cases) area around the clavicle button can be observed, but most of the time it is asymptomatic.
AC arthritis (8/32 HP, 5/19 TR) is seen in plain radiographs in both group, but it seems to be related to initial injury and the patients did not feel the arthritic symptom. Asymptomatic AC joint degeneration is frequent and does not always correlate with the presence of symptoms.19)
Our study has limitations that are inherent to retrospective, nonrandomized studies. Even though we believed the slow restoration of ROM gain is mainly caused by discrepancy of rehabilitation programs between two groups, however we could not eliminate other factors such as operative times, incision length or operative procedure itself.
Conclusion
AO hook plate fixation and TightRope fixation for acute unstable AC joint dislocation result in no significant difference in clinical outcome, reduction of the AC joint and arthritic change of AC joint. And ROM recovery time is different but it is depends on rehabilitation date after surgery. Therefore both Hook plate and TightRope fixation could be a recommendable treatment option in acute unstable AC joint dislocation.



 XML Download
XML Download